Computed tomography (CT) is the standard diagnostic test for evaluating cross-sectional, two– or three-dimensional images of the body(1).
Healthcare providers often debate whether CT or magnetic resonance imaging (MRI) of the orbit is more effective in identifying orbital pathology symptoms.
Some experts state that age, clinical suspicion, possible radiation tolerance, and systemic status may influence clinicians when choosing from either modality.
Experts have suggested that CT should be the primary diagnostic imaging modality for the orbit (eye sockets)(2). Clinicians may order MRI orbit tests as a secondary diagnostic tool when the CT does not entirely clarify the optic nerve’s relation.
CT Physics
Content CT is a technology that utilizes X-ray radiation beams and a range of radiation detectors surrounding the part under examination. CT works as explained by two principles:
- Radiologists acquire images by the rapid rotation of the X-ray tube 360° around the patient. The technician then measures the radiation by a ring of sensitive radiation detectors located on the gantry around the patient.
The technician reconstructs the final image in a 2D or 3D manner from multiple X-ray projections.
- CT works by measuring different absorption values of tissues after their exposure to X-ray. As the X-ray beam traverses the body, it weakens, depending on the density of the tissues it passes through.
Preset formulas convert these absorption values into gray-scale units. The technicians can show the reconstructed image on a screen, review it on a picture archiving and communication system (PACS), or print it on film, mainly composed of silver halide and silver bromide salts(3-6).
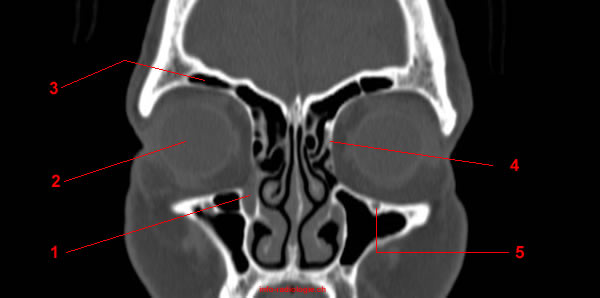
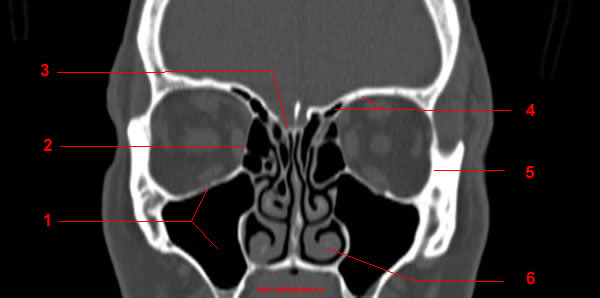
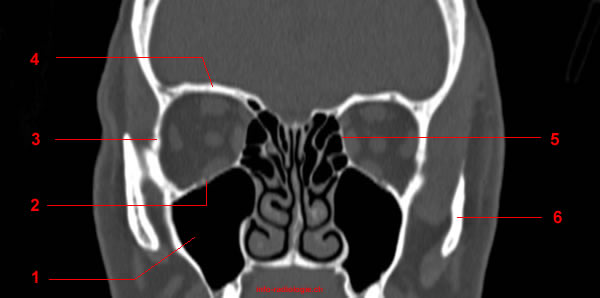
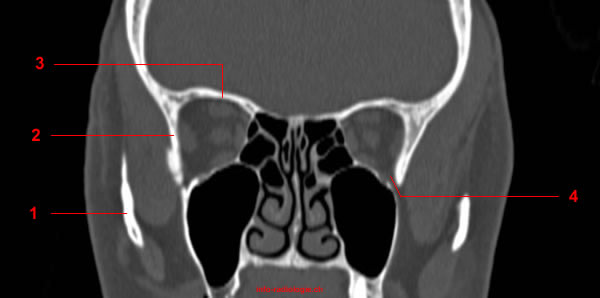
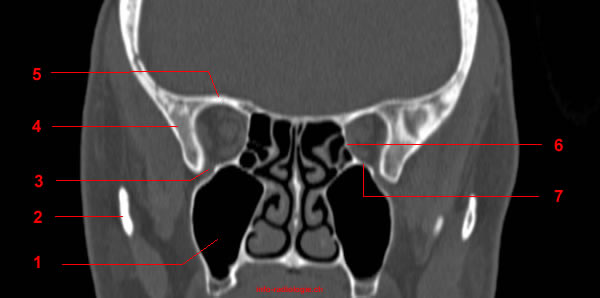
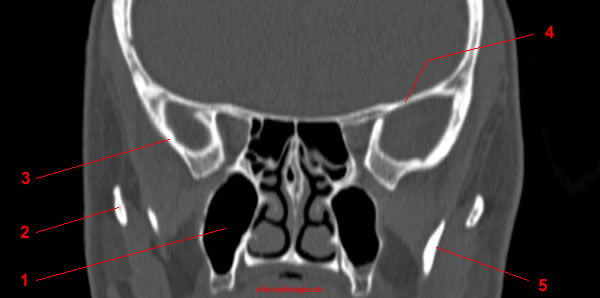
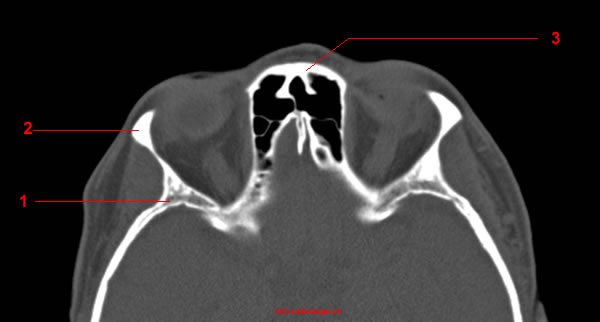
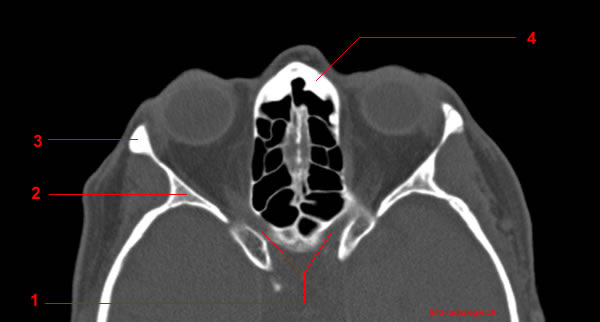
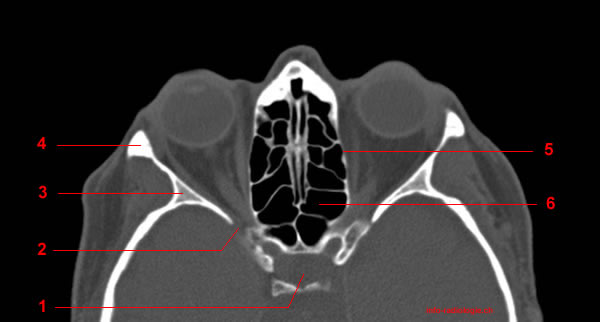
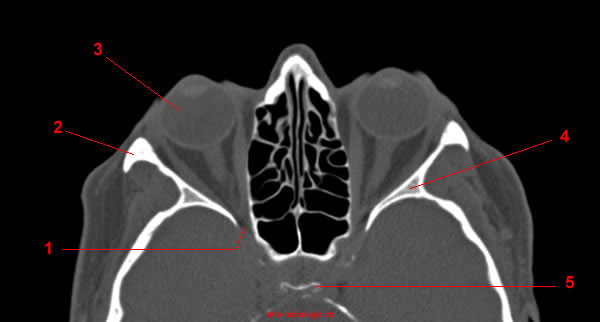
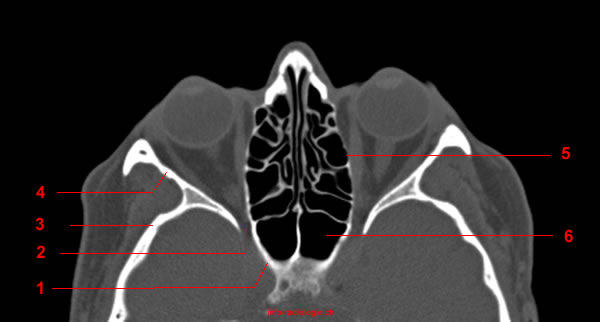
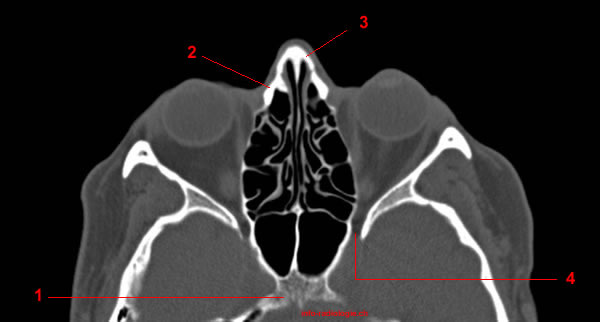
Imaging of the Orbit
The orbit is the site of many pathologies of diverse etiologies (causes of disease). Radiologists must tailor their imaging modalities to the symptoms and clinical findings(7).
The most common clinical indications for orbital imaging include the following:
Exophthalmos
Proptosis or exophthalmos is the bulging condition of the eye. The eyeball’s protrusion may result from a wide range of potential vision- or life-threatening pathologies(8).
Besides CT imaging features, other factors crucial in establishing the disease’s underlying causes include the patient’s clinical history and the associated physical exam findings.
Enophthalmos
Enophthalmos refers to the sinking of the eyeball into the bony cavity protecting the eye.
Physical examinations combined with thin-section CT scanning in the axial and coronal planes provide the operative plan for treating enophthalmos(9).
Diplopia
Diplopia refers to seeing double. This condition may be due to ocular misalignment, which disappears when either eye is blocked.
The condition may also be due to an optical problem. In this case, it is called monocular diplopia and does not disappear with monocular viewing(10).
Patients with ocular misalignment may have severe pathology. Thus, they must seek evaluation systematically and thoroughly in order to expose all potentially serious cases.
Leukocoria
Leukocoria means “white pupil” or “cat’s eye pupil.” This condition is an abnormal pupillary reflex more clearly seen in mydriasis or photography. Leukocoria may often be the first sign of a range of severe intraocular disorders(11).
If a child is suspected of leukocoria, experts may avoid evaluating them using CT. This method exposes the child to high radiation. Still, CT can be useful if intraocular calcification is doubtful.
Diminished Vision
Visual loss is common after head trauma, although diagnosis is often made late. The fact that trauma patients may be unconscious and unable to provide a clinical history complicates clinical assessment of such conditions(12).
Experts suggest that patients who suddenly experience visual loss after blunt head trauma undergo a CT scan of the optic canal region(13).
Craniofacial Developmental Anomalies
Craniofacial developmental anomalies are deformities that affect the head and facial bones. Such conditions include cleft lip and palate and craniosynostosis (a congenital disability in which the bones in a baby’s skull join together prematurely).
Craniofacial malformations that occur because of abnormal development comprise over one-third of all congenital disabilities(14).
Experts may recommend CT imaging techniques to evaluate congenital and developmental anomalies of the midface and skull base. Such techniques may include multiple detector spiral imaging with multiplanar reconstructions(15).
Epiphora
Epiphora is the excessive production of tears in one or both eyes. This condition affects children and adults(16).
CT and MRI scans are among the excretory tests clinicians may perform in patients presenting with epiphora(17).
CT delineates bony abnormalities better than MRI, allowing determination of the cribriform plate’s level (the bone that transmits the olfactory nerves that carry the sense of smell).
In assessing nasal and sinus diseases, radiologists use both CT and MRI machines(18).
Reference:
• Harnsberger HR, Osborn AG, Ross JS, Moore KR, Salzman KL, Carrasco CR, Halmiton BE, Davidson HC, Wiggins RH. Diagnostic and Surgical Imaging Anatomy: Brain, Head and Neck, Spine. 3rd ed. Salt Lake City, Utah. Amirsys. 2007.
• Bourjat P, Veillon F. Imagerie radiologique tête et cou. Paris, Vigot. 1995.
• Gouazé A, Baumann JA, Dhem A. Sobota. Atlas d’Anatomie humaine. Tome 3. Système nerveux central, système nerveux autonome, organe des sens et peau, vaisseaux et nerfs périphériques. 1er éd. Paris, Maloine. 1977.
• Kahle W, Cabrol C. Anatomie. Tome 3: Système nnerveux et organe des sens. 1er éd. Paris, Flammarion. 1979.