

This webpage presents the anatomical structures found on shoulder X-ray.
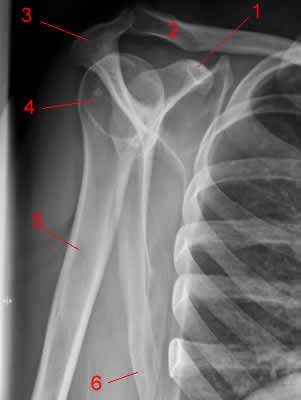
Shoulder X-ray, AP projection
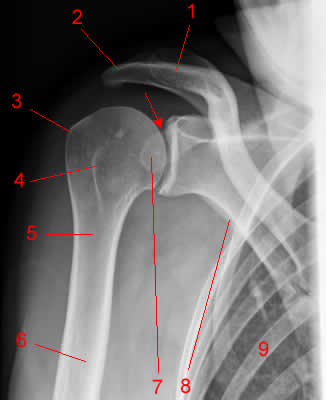
Shoulder X-ray: lateral view
Experts agree that imaging assessment of shoulder disorders must begin with radiographs. Radiologists have developed several radiographic examinations to best show the areas affected by specific clinical disorders(1).
Grashey View
This projection is a true anterior-posterior (AP) view of the shoulder. The Grashey view involves angling the beam laterally or rotating the patient posteriorly(2).
These adjustments remove the view of the overlap between the humerus and the glenoid. The removal allows better evaluation of joint congruity, humeral head subluxation, and the glenohumeral cartilage space(3).
Adding abduction and weight gives an axial load to the shoulder joint that may increase the ability to demonstrate articular cartilage loss(4).
Axillary View
Clinicians typically use the axillary view in evaluating subluxations and dislocations of the humeral head, generally centered on the glenoid and round in contour. This projection is also useful in evaluating osseous Bankart lesions(5).
The glenoid is a cavity or joint in the shoulder.
West Point View
This view is a modified axillary projection, with the advantage of demonstrating the anterior aspect of the glenoid.
Some patients with an acute shoulder injury may find it challenging to comply with this projection(6). Still, this projection can improve the detection of a bony Bankart lesion, which occurs when part of the glenoid bone gets broken off with the anterior labrum tissue.
Retrospective studies have documented the West Point view as one of the best projections to detect bony Bankart lesions(7).
Scapular Y-View
The scapular “Y” projection is useful in evaluating anterior and posterior shoulder dislocations. Clinicians highly recommend this view for the minimal shoulder motion necessary to obtain it(8).
Information from comparing the axillary and scapular Y-views demonstrates no significant difference in detecting abnormalities. The Hill-Sachs lesion is an exception, which the Y-view detects better than the axillary view(9).
The Y-view is also useful in determining acromial morphology and detecting fractures of the acromion, the coracoid process, and the scapula(10).
Supraspinatus Outlet View
This projection is useful in evaluating the acromion process and subacromial abnormalities. Such conditions include osteophytes (bony lumps) that may cause impingement (a painful condition that occurs when tendons, nerves, or adjacent structures experience pressure)(11).
Despite its similarities to the Y-view, the supraspinatus outlet view is different because of caudal tube angulation. Caudal angulation involves directing the X-ray beam caudally or toward the body’s posterior(12).
Stryker Notch View
When clinicians combine the Stryker notch view with an AP internally rotated view, the projection is potentially the most sensitive technique for evaluating a Hill-Sachs deformity(13).
Radiographic Features of Specific Conditions
Clinicians can classify shoulder disorders based on the areas affected.
Alignment
Proximal Humerus Fractures
The Neer system, published in 1970, is the standard classification system that clinicians use today in accurately describing a fracture(14).
Fractures of the proximal humerus occur between one or all of these four primary segments:
- The articular segment (at the level of the anatomic neck)
- The greater tuberosity
- The lesser tuberosity
- The humeral shaft (at the level of the surgical neck)
The original Neer classification describes fractures as displaced if a segment separates by more than 1cm or angulates by more than 45 degrees from other fragments.
Glenohumeral Joint Dislocations
The Journal of Emergency Medicine classifies shoulder dislocation as the most common large joint dislocation(15).
Furthermore, anterior shoulder dislocations are the most common type, accounting for 95% of all shoulder dislocations(16).
Meanwhile, posterior shoulder dislocations make up less than 5% of all shoulder dislocations. Inferior or subglenoid dislocation (luxatio erecta) is extremely rare, occurring in approximately 0.5% of cases(17).
Patients who may have shoulder dislocation typically undergo pre-reduction radiographs to confirm the condition and identify related fractures(18).
Bone Density
Avascular Necrosis
Avascular necrosis (AVN) is the loss of blood supply to the bone. Three common AVN etiologies include post-traumatic sequela, corticosteroid use, and sickle cell disease(19).
AVN’s typical radiographic findings depend on the condition’s stage, which may range from subtle lucency (an area that allows X-rays through tissues) and sclerosis (skin hardening) to fragmentation and subarticular collapse. Further possibilities include arthritis and joint destruction in the final stages.
Cartilage Spaces
Osteoarthritis
The shoulder is a non-weight bearing joint. Hence, primary osteoarthritis of the shoulder joint is uncommon. Underlying causes include prior trauma, systemic arthritis, congenital malformations, chronic rotator cuff tear, and acromegaly(20).
Osteoarthritis usually involves asymmetric cartilage space narrowing. Osteophytes that arise from the glenoid rim and the humerus’ anatomic neck are also a characteristic of the condition. In acromegaly, the osteophytes are typically large(21).
Soft Tissues
Calcific Tendonitis
Radiographers have detected periarticular calcification in symptomatic and asymptomatic individuals. One study lists the shoulder as the most common site of calcific tendonitis or bursitis, comprising half of the supraspinatus tendon cases(22).
Radiography can localize calcification to a particular tendon. Imaging the condition can also indicate whether the process is chronic or acute.