Radiologists perform ankle imaging to assess injuries of the foot and ankle anatomy. Experts analyze the different imaging techniques to identify better diseases associated with the foot and ankle, including diabetic foot ulcers and abnormal growths in the foot and ankle(1).
How Does Ankle MRI Work?
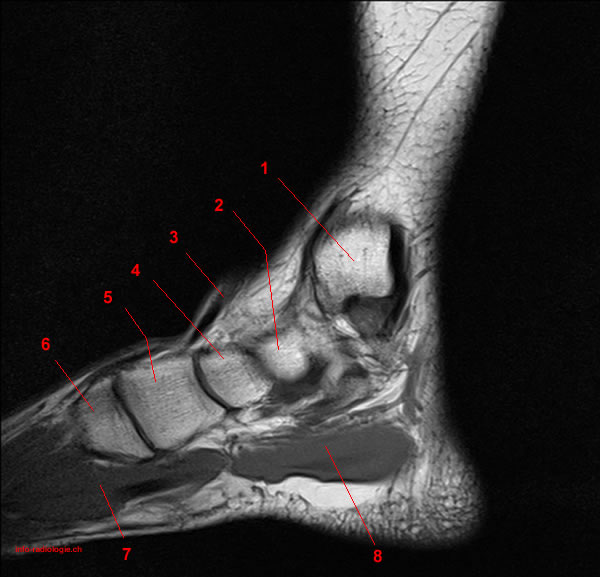
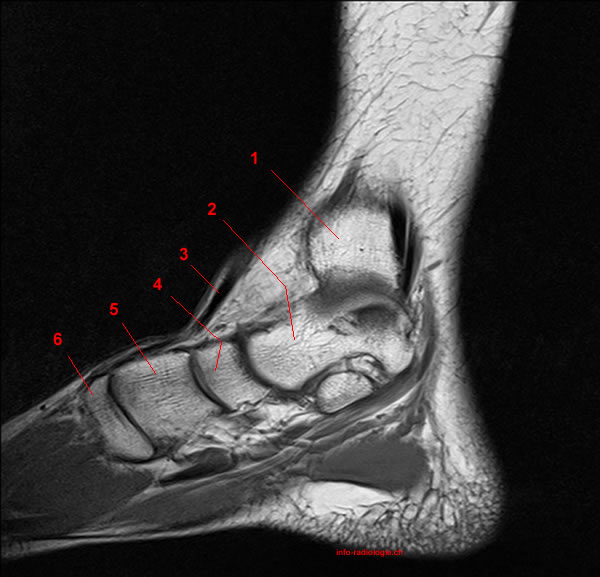
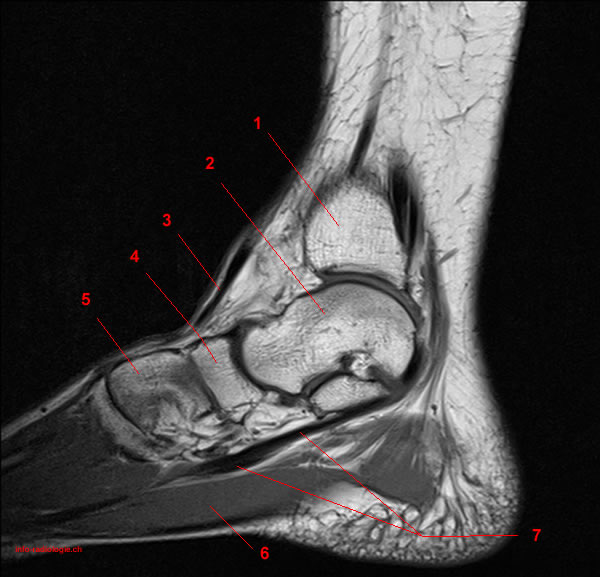
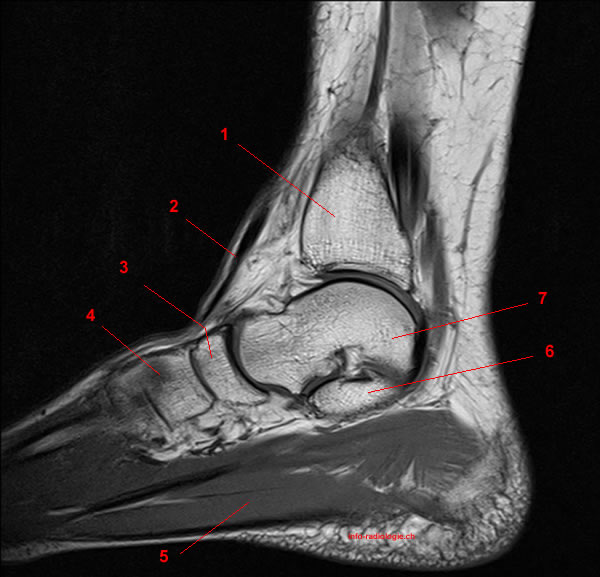
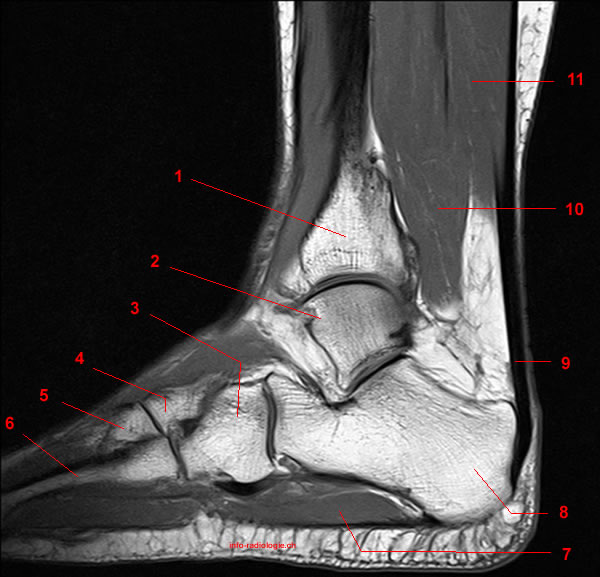
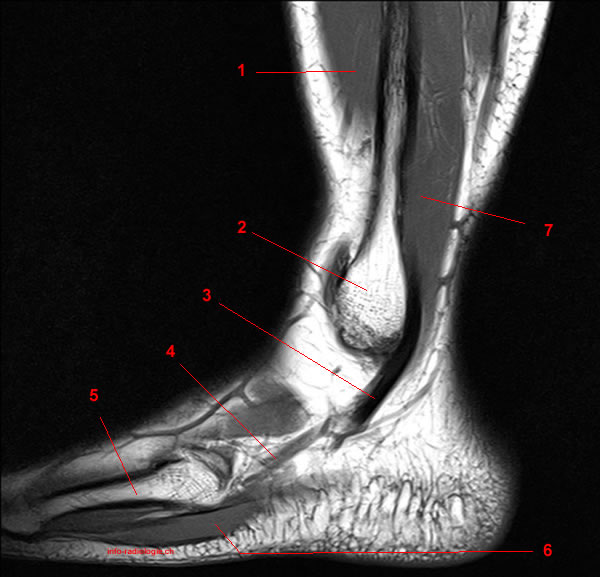
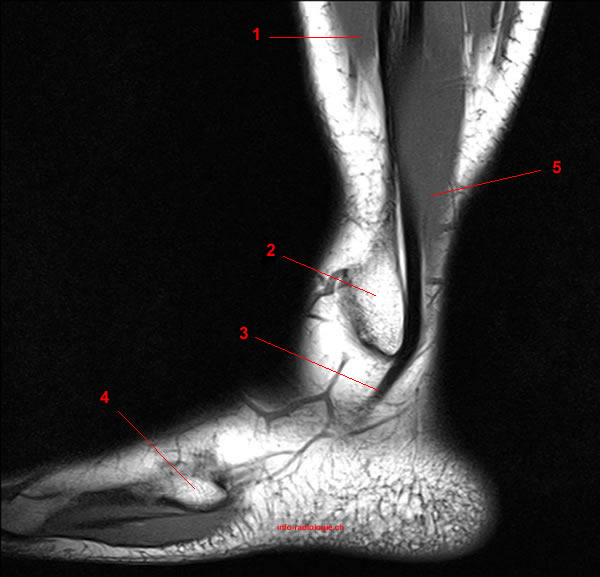
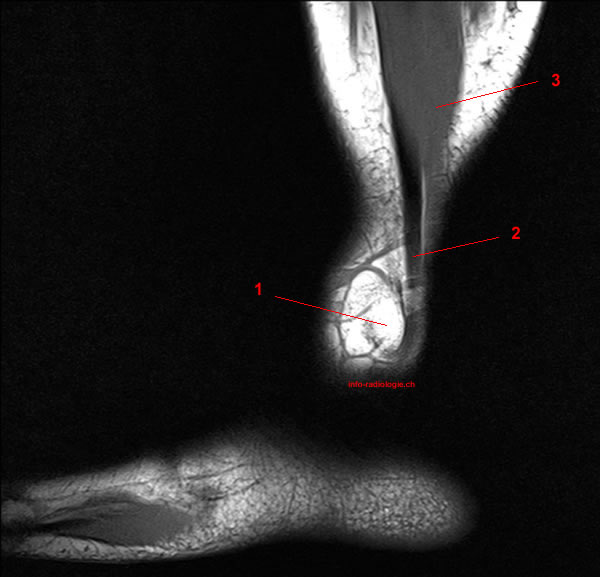
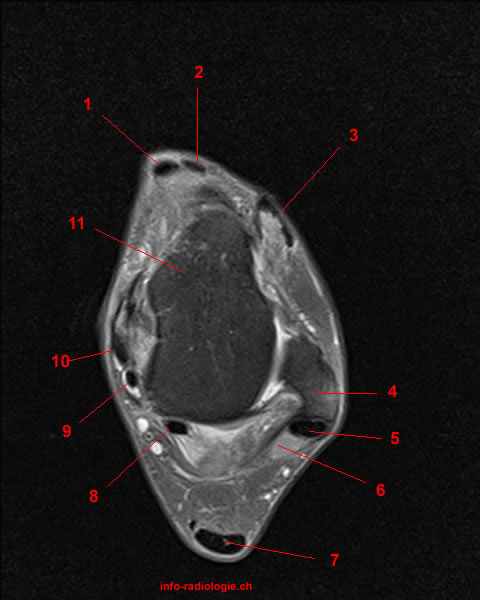
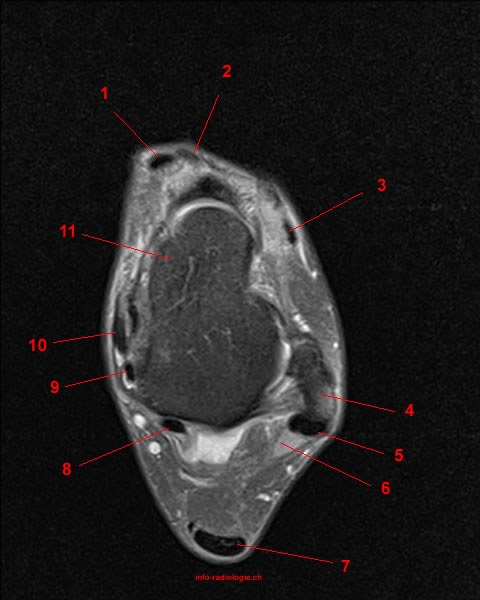
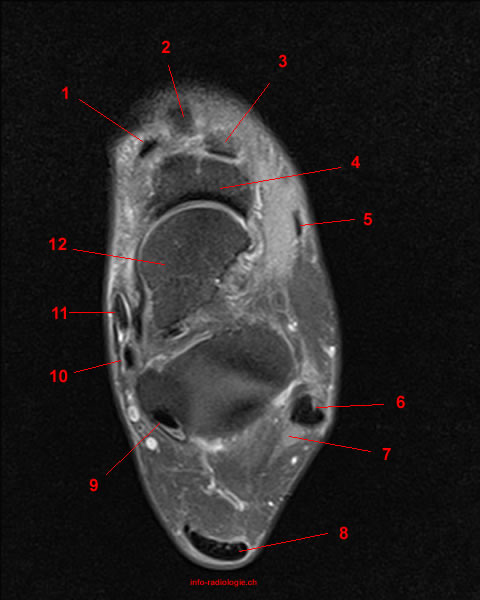
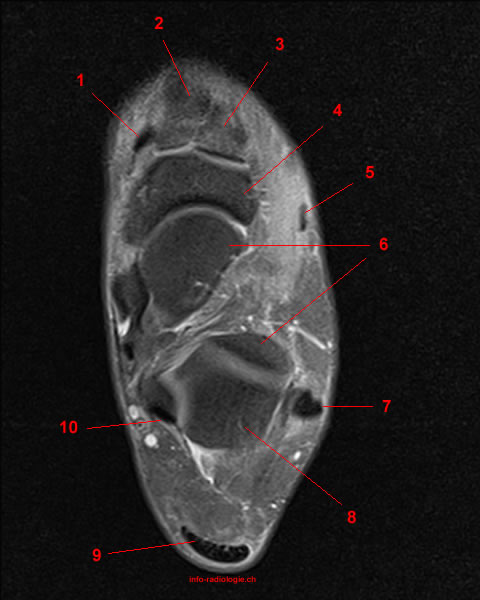
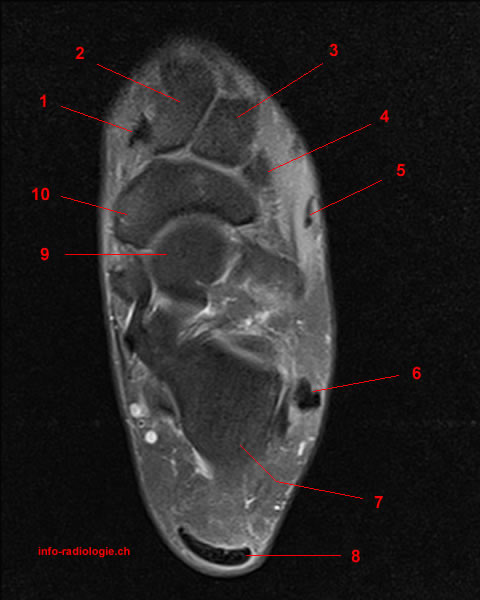
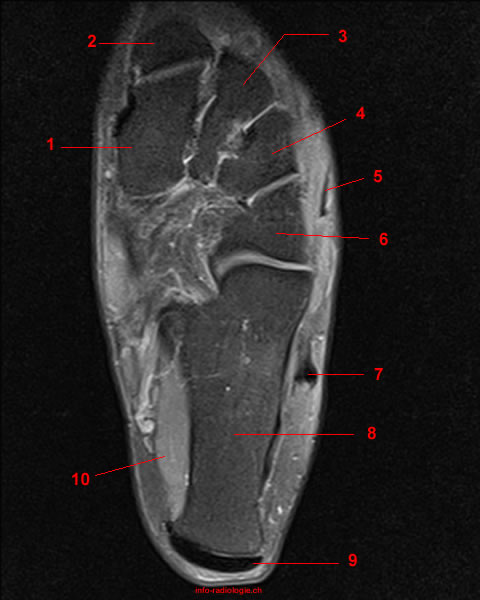
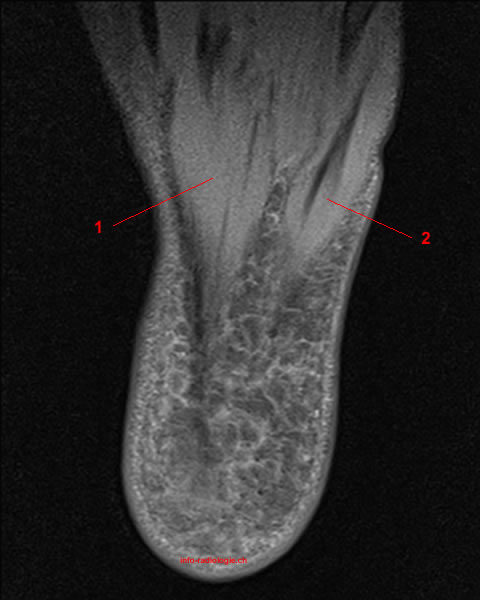
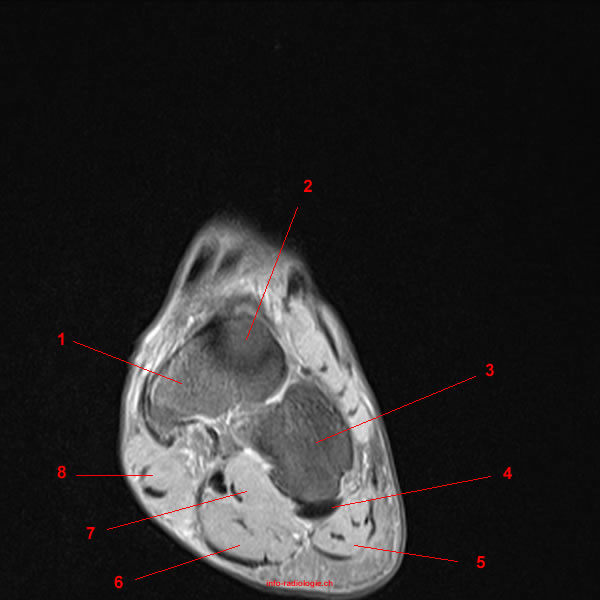
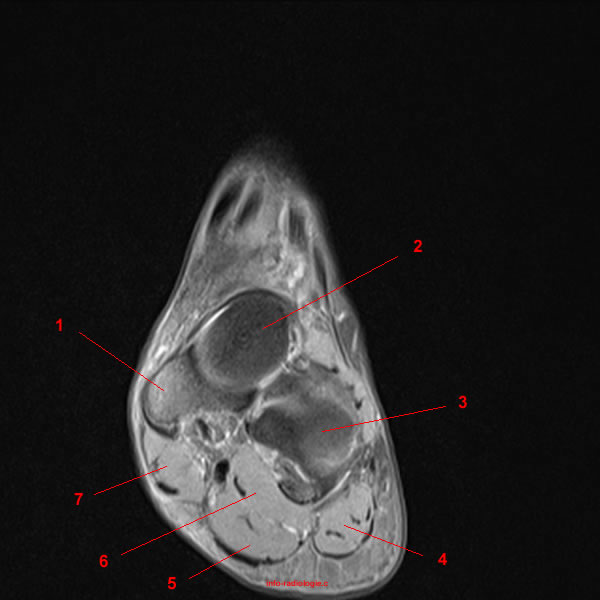
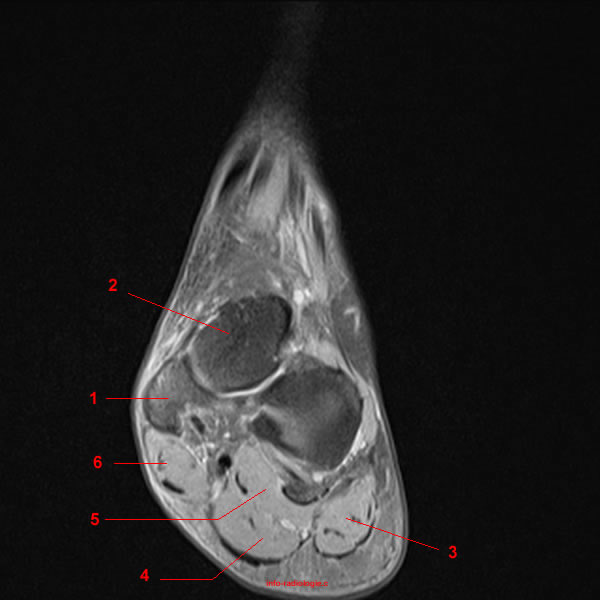
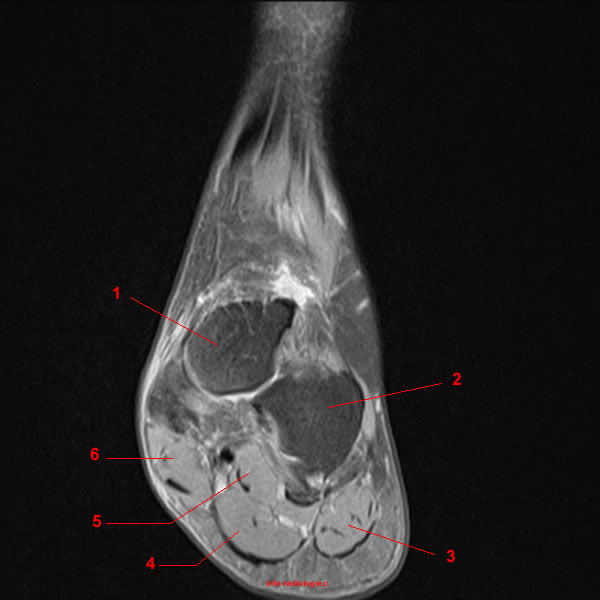
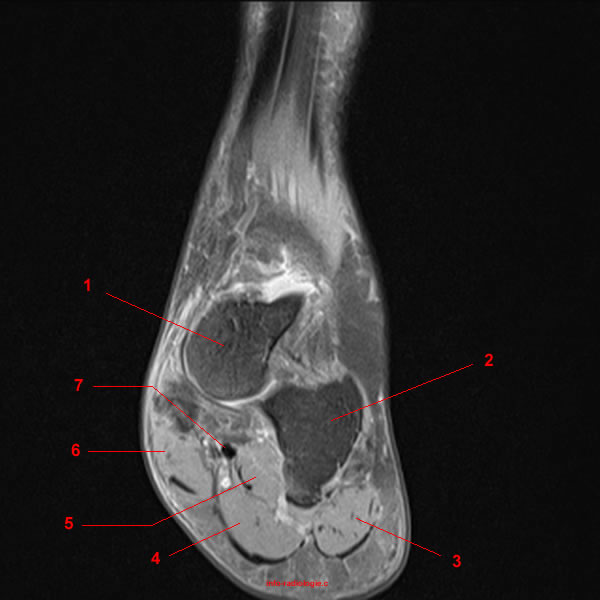
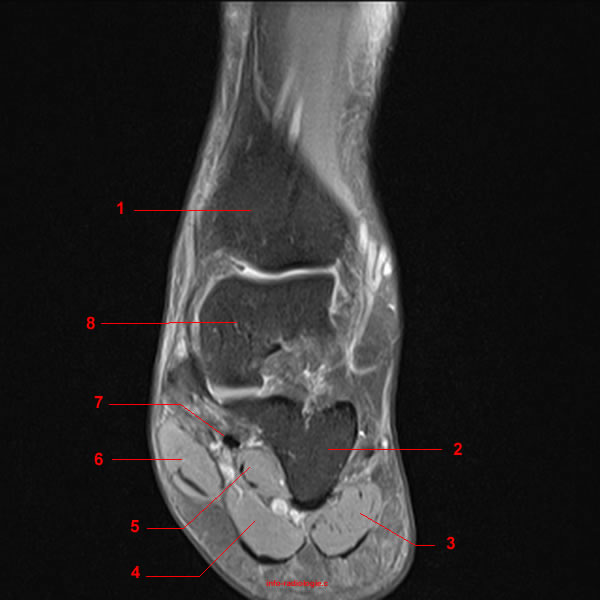
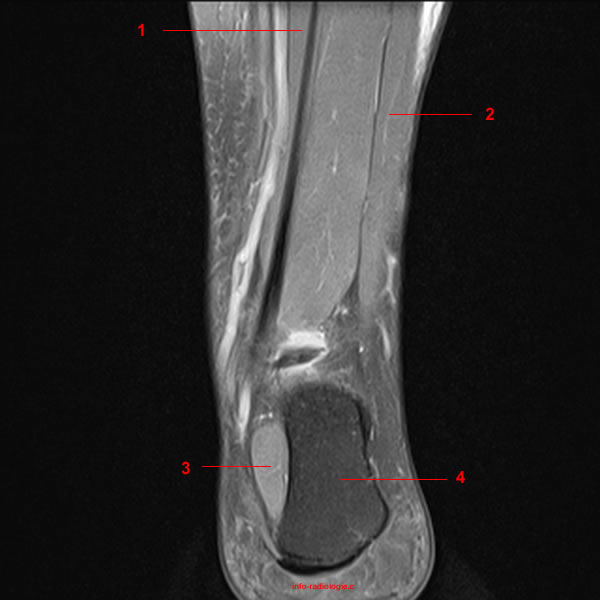
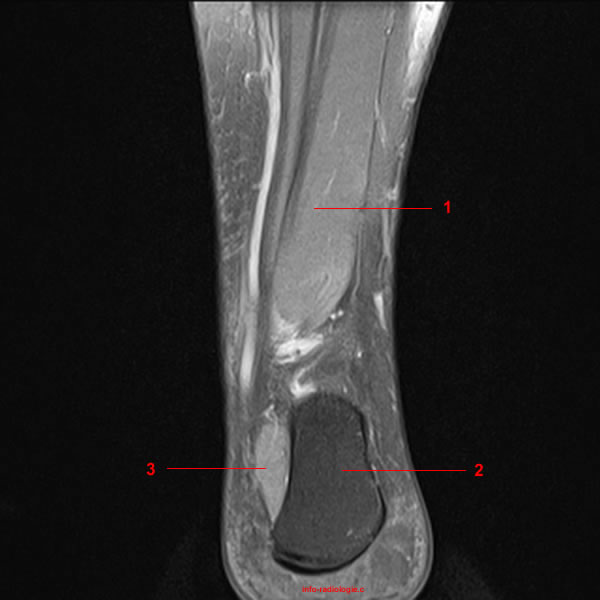
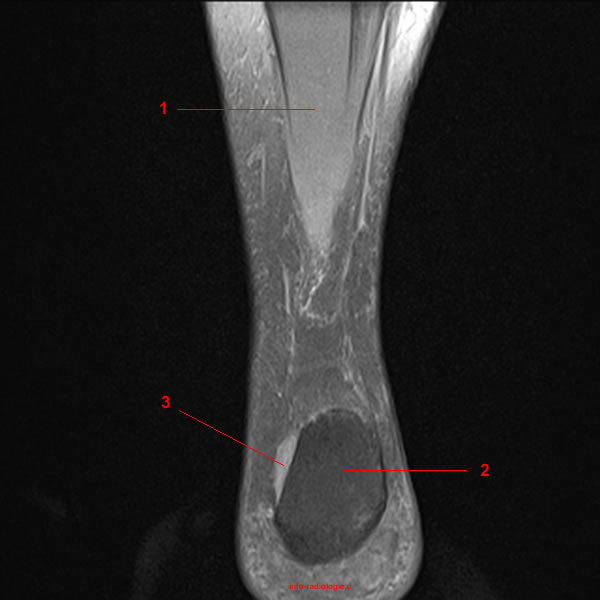
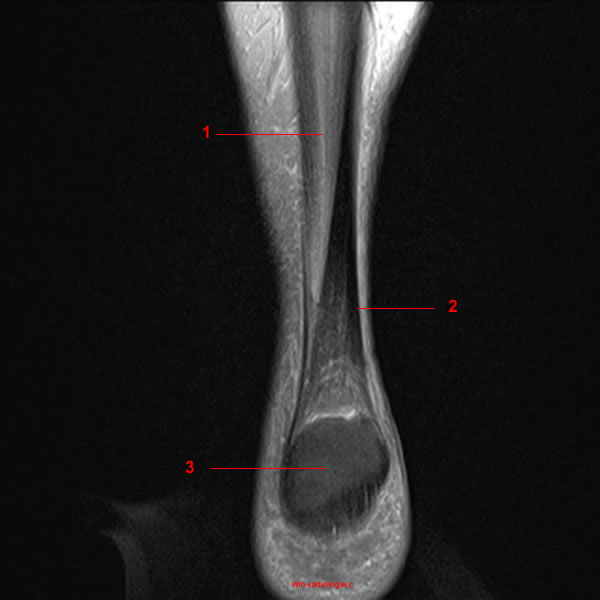
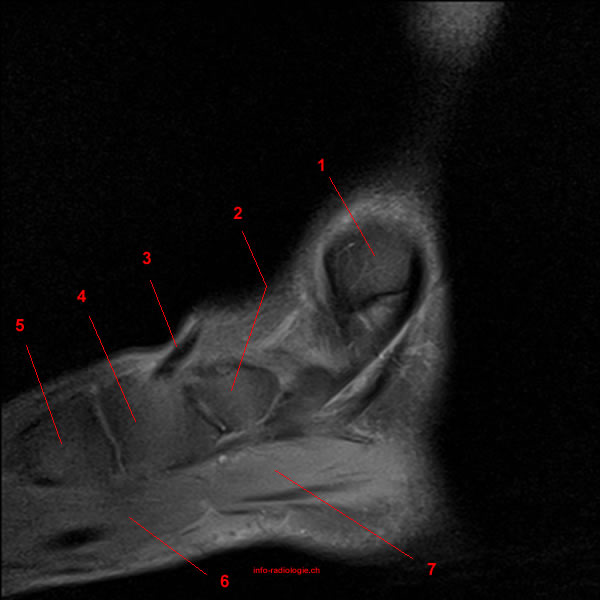
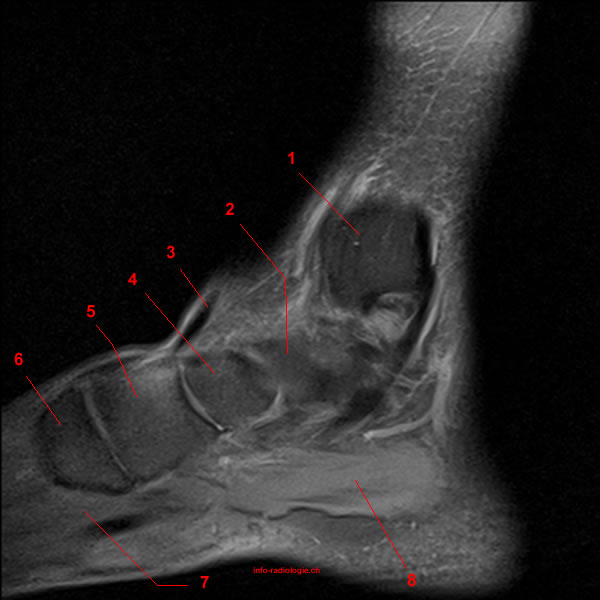
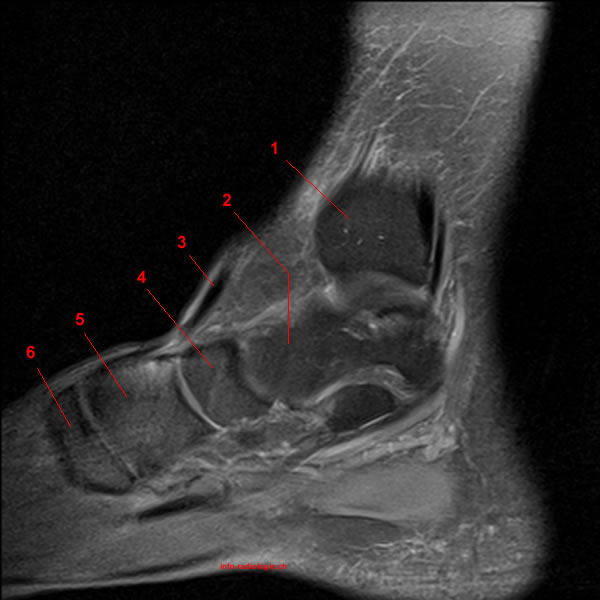
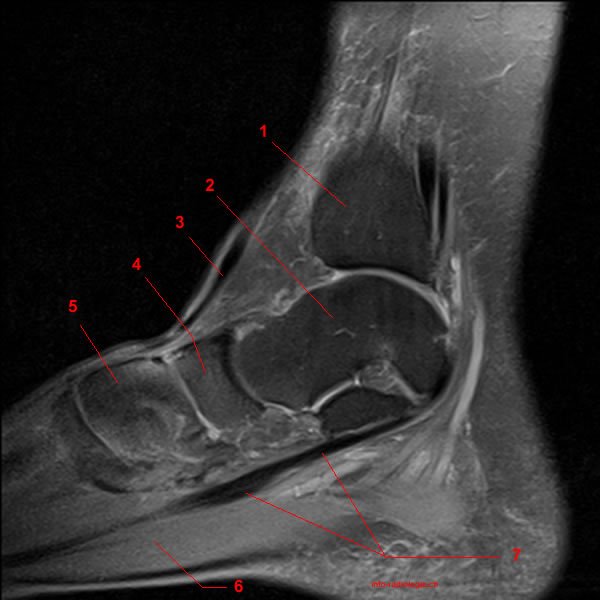
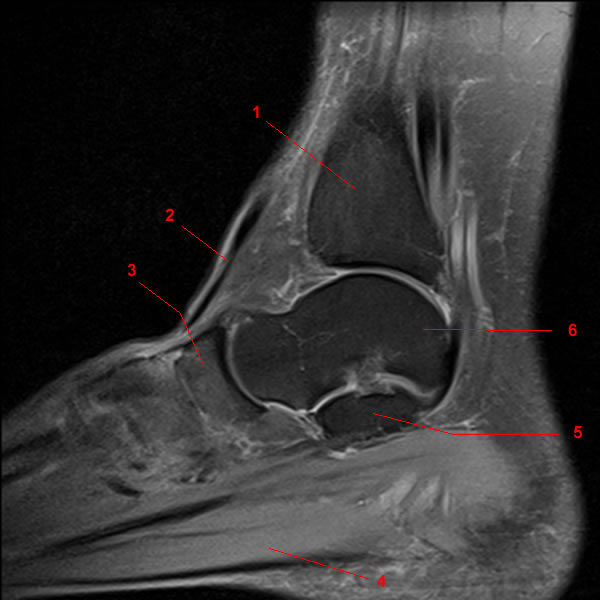
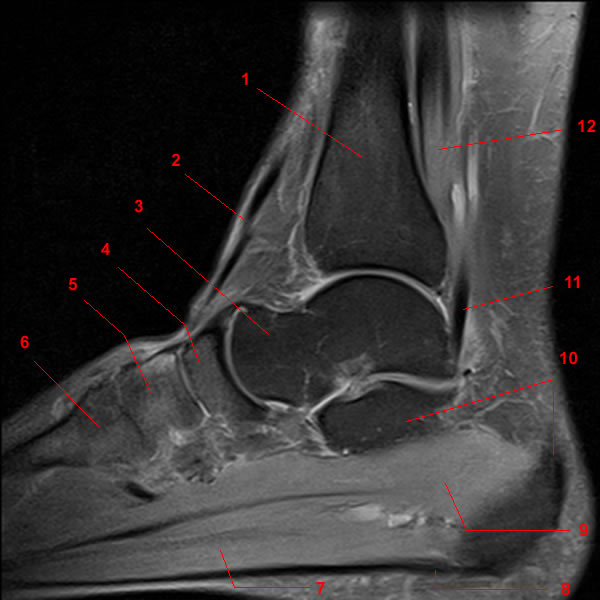
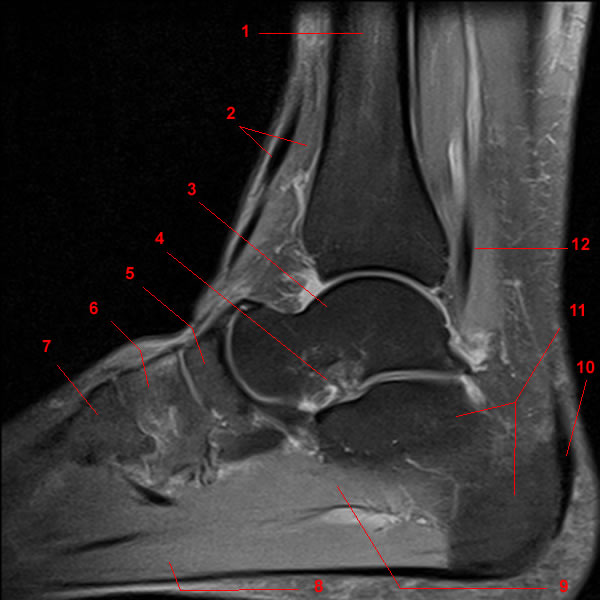
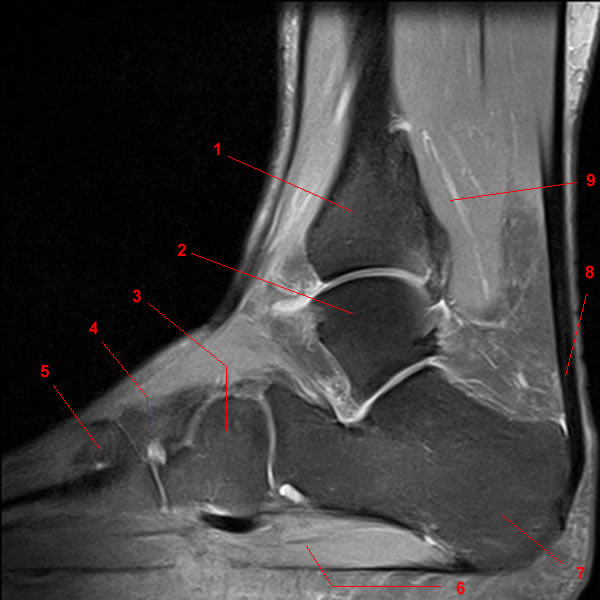
Routine ankle magnetic resonance imaging (MRI) tests involve taking images of the foot and ankle in the axial, coronal, and sagittal planes parallel to the tabletop(2).
Axial images are parallel to the long axis of the metatarsal (mid-foot) bones. Coronal images are perpendicular to the long axis of the metatarsals. Meanwhile, sagittal images are lateral, meaning they divide the foot into its left and right sides).
Compared to CT scans, ultrasounds, or X-rays, MRI tests give doctors a more detailed look at soft-tissue structures. The images allow the experts to assess a variety of soft-tissue disorders of ligaments and tendons.
During an MRI test, patients are supine (lying face upward) with their foot in about a 20-degree plantar flexion (moving the foot downward away from the body, the way a ballet dancer stands on their toes). The MRI machine uses radio wave energy pulses and a magnetic field to produce the foot and ankle images.
The imaging process allows the magnetic field to find changes in the organ and tissue structures, identifying any sprains, ruptures, dislocations, or synovial disorders (conditions that affect the thin tissue layer lining the joints).
MRI pictures are digital, allowing other doctors to review the scanned images for further study remotely.
For physical copies of the MRI pictures, technicians may use a contrast material during the MRI test to highlight specific structures. Contrast materials are substances that help show areas of infection or inflammation by making structures appear more clearly.
Osseous Lesions
Ankle MRI includes assessments of the foot’s bone structures. The foot has 26 bones (tarsal, metatarsal, and phalanges), which subdivide into groups, known as the hindfoot, midfoot, and forefoot(3).
Assessing these parts help doctors identify the following diseases:
- Osteonecrosis: Also known as avascular necrosis, this disease is the death of bone tissue due to a lack of blood supply. Osteonecrosis can lead to tiny breaks in the bone and the bone’s eventual collapse(4).
Ankle and foot osteonecrosis typically occurs in the talus due to talar neck fractures with a vascular compromise of the bone at the sinus tarsi level (tube between the ankle and heel)(5).
- Osteochondral Fractures: Experts consider osteochondral fractures as injuries that damage the cartilage. These conditions may also affect the underlying subchondral bone (bone sitting underneath cartilage in a joint)(6).
Ankle osteochondral fractures usually appear in the talar dome, most frequently in the middle third of the lateral border and the posterior third of the medial border(7).
- Stress Fractures and Acute Posttraumatic Fractures: A fracture is a break in the bone that may occur after falls, sports injuries, or vehicular accidents. Experts find that MRI is more sensitive than conventional radiography. MRI can also be more specific than bone scintigraphy in detecting occult fractures(8).
- Bone Contusion: Bone contusions or bone bruises are related to the trabecular bone (spongy, light, and porous bone) and edema (swelling) or hemorrhage within the bone marrow. Constant stress placed on a contused bone may lead to complete fracture(9).
Tendon Injuries
Tendon injuries have six categories: dislocation, entrapment, peritendinosis, rupture, tendinosis, and tenosynovitis(10).
These conditions often coexist and overlap in their clinical, gross, and histologic manifestations, making them indistinguishable at MRI tests(11).
Some conditions that doctors can assess from an MRI test may include:
- Flexor Hallucis Longus Tendon Injuries: The flexor hallucis longus (FHL) tendon is susceptible to injuries along the entire course, from the ankle’s posterior aspect to the insertion into the great toe’s distal phalanx base(12).
Experts note various lacerations, ruptures, longitudinal splits, and stenosing tenosynovitis among the injuries.
MRI tests may find FHL injuries better through axial and sagittal MR images(13).
- Peroneal Tendon Injuries: Injuries to the peroneal tendons include dislocation, peritendinosis, rupture, tendinosis, and tenosynovitis(14).
MRI scans characterize findings of peritendinosis as scarring around the tendons. Meanwhile, tenosynovitis manifests as the fluid within the common tendon sheath(15).
- Posterior Tibial Tendon Dysfunction: Posterior tibial tendon dysfunction is primarily soft tissue tendinosis of the posterior tibialis. This condition may lead to altered foot biomechanics. Most experts agree that it is a progressive disorder(16).
- Achilles Tendon Injuries: Achilles tendon injuries are the most common tendon ruptures of the foot are. These injuries usually occur in individuals who are only intermittently active(17).