

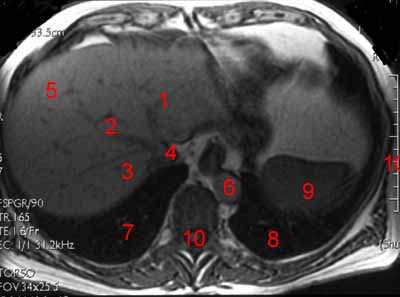
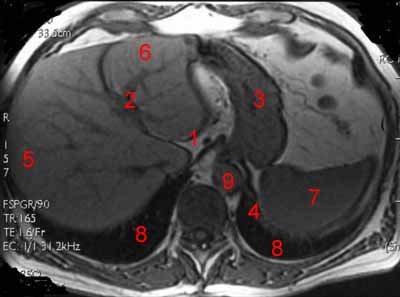
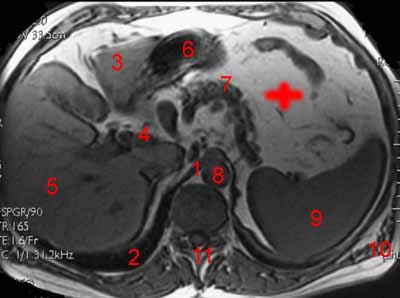
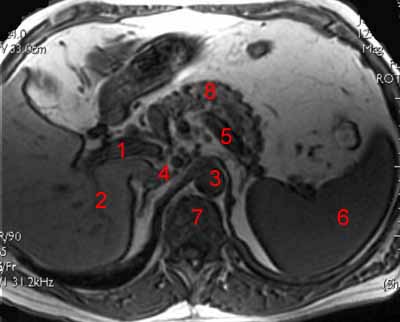
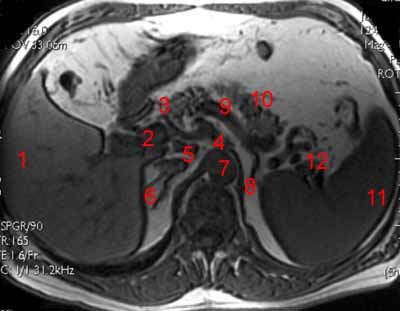
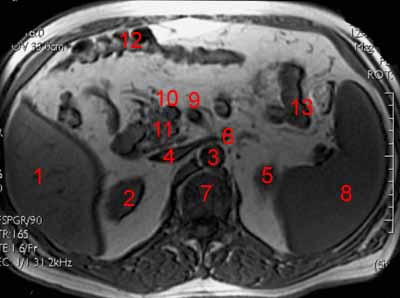
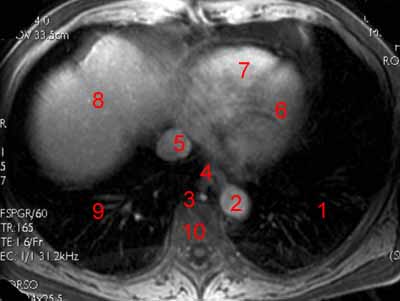
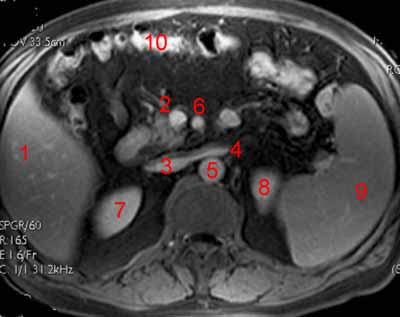
This photo gallery presents the anatomy of the abdomen by means of MRI.
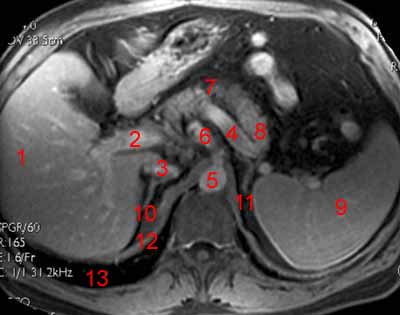
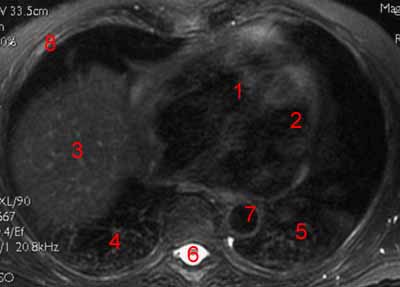
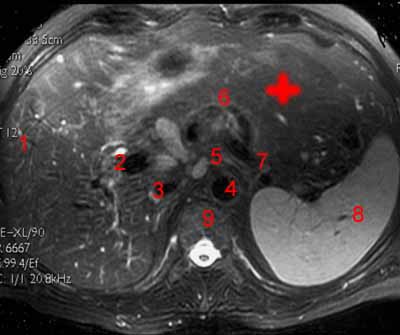
Axial T1-weighted images
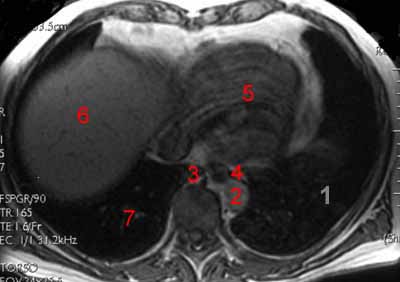

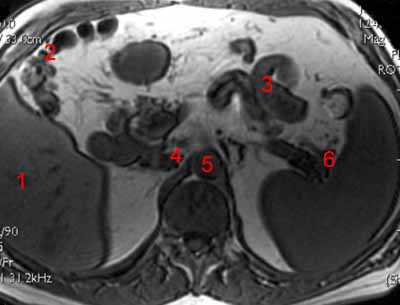

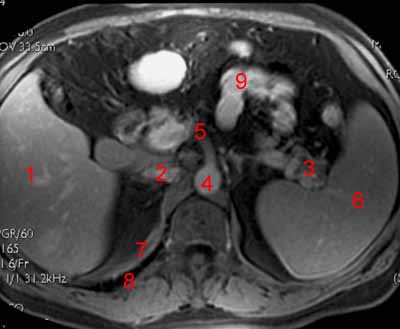
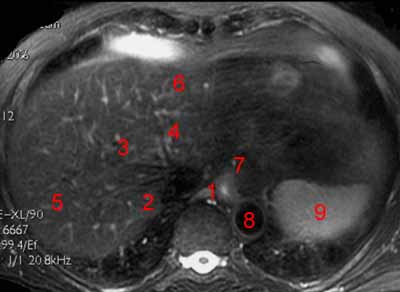
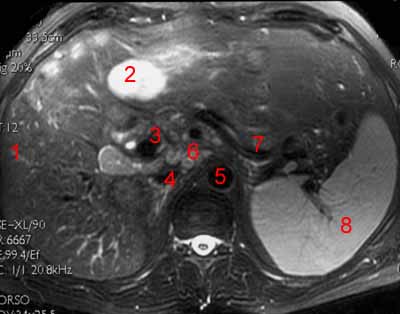
Axial T1-weighted fat-suppressed images after injection of contrast
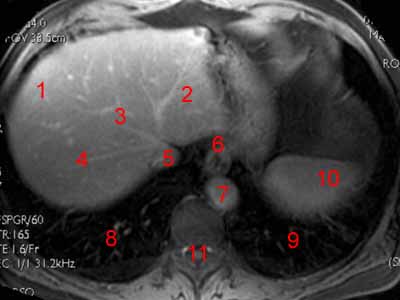
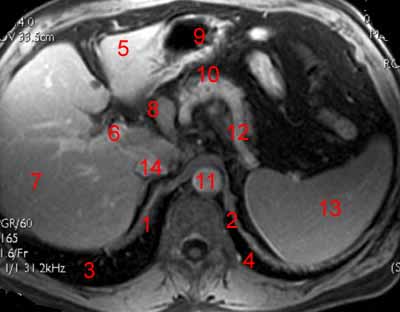
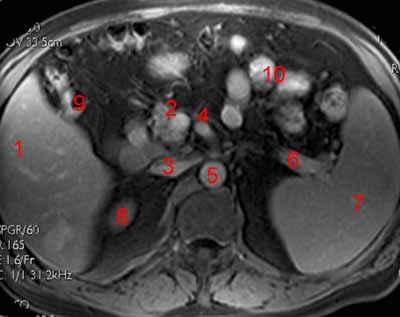
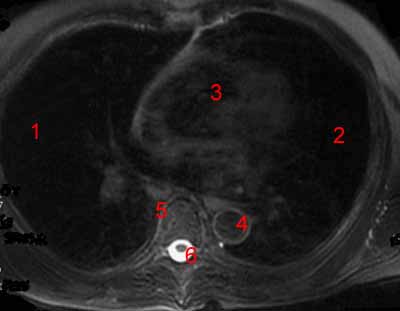
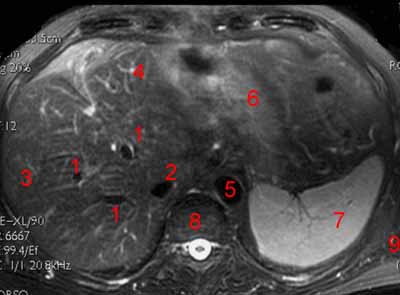
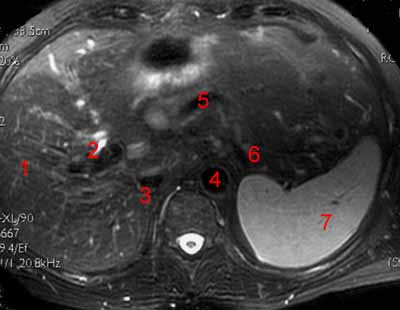
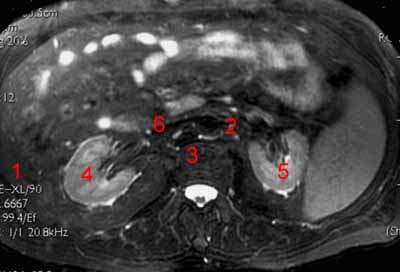
Axial T2-weighted fat-suppressed images

Radiologists routinely use magnetic resonance imaging (MRI) to diagnose many upper abdominal tumors(1).
MRI is non-ionizing, making the modality more advantageous over other imaging sequences that involve higher radiation exposure. MRI can provide practical information and better soft tissue resolution than computed tomography (CT)(2-3).
The primary advantage of MRI in treating upper abdominal malignancies, particularly liver cancers, lies in CT’s difficulty to detect and characterize tumors. Additionally, MRI can better characterize some organs at risk, such as the common bile duct and distal biliary tree(4).
Upper abdominal organs are also subject to respiratory motion, bowel peristalsis, and daily positional variation. These conditions are suitable for online MRI guidance and adaptive radiation therapy(5-8).
The commercial availability of MRI-guided treatment units has increased. This boost in availability amplified the focus on online MRI-guided radiation therapy (MRgRT) for treating pancreatic cancer, liver cancer, kidney cancer, adrenal cancer, and upper abdominal metastases(9-11).
MRI simulation and online MRgRT are becoming more commonly used to identify gross tumor volume (GTV) and organs at risk (OAR). These modalities are useful in upper abdominal radiation planning and treatment (especially for pancreas and liver cancer)(12).
Experts have used two commercially integrated online MRgRT systems for treating patients with upper abdominal tumors:
- A 0.35T MRI scanner combined with 3 Cobalt-60 teletherapy heads or a 6X FFF linear accelerator and multileaf collimators (MRIdian, ViewRay)
- A 1.5T MRI scanner combined with a 6X linear accelerator (Unity MRLinac, Elekta AB)(13-14).
Other online MRgRT systems are in development. Among these systems are the 1.0T Australian MRI LINAC System (Australian MRI-LINAC Program, Sydney, Australia) and the 0.6T Aurora-RT System (MagnetTx, Edmonton, Alberta, Canada)(15-16).
The accurate definition of the GTV and OARs ensures safe radiation treatment. Precise definitions can realize the potential of real-time MRI-based image guidance and adaptive treatment planning(17).
Meanwhile, several standard tissue contouring atlases for radiation planning exist. However, they are CT-based(18-19).
Professionals expect online MRgRT to increase the accuracy and precision of radiation treatment delivery. The method also improves adaptive radiation therapy and allows response assessment throughout treatment(20).
With the increasing use of MRI, standardization of target volume and OAR definition via MRI have become necessary.
Standardization improves the consistency of radiation treatment plans. Having standard definitions also facilitates high-quality collaborative studies and OAR dose-volume-toxicity analyses(21).
Many radiation oncologists have not routinely used MRI for simulation or guidance. Most radiation therapists also lack training in MRI anatomy(22).
An MRI-based atlas is useful in defining commonly used vocabulary (such as liver segments). An atlas can also define OARs that CT-based radiation therapy may not have consistently visualized or contoured.
Liver
Unenhanced MRI-defined GTV connects better with the pathologic GTV than other imaging modalities among patients with primary and secondary liver tumors. Other modalities include CT or positron emission tomography(23).
MRI in liver imaging has superior soft-tissue contrast. This advantage allows better detection and characterization of malignant and benign focal liver lesions(24).
The development of liver-specific MRI contrast agents (substances that make images clearer) has further improved MRI diagnostic yield in detecting and characterizing lesions.
It is necessary to detect focal liver lesions early, particularly malignant ones. Patients’ survival rates improve upon the resection of liver metastases of some malignancies, such as colorectal cancer(25).
Spleen
The spleen is an intraperitoneal (within the abdomen) organ located in the abdomen’s upper-left quadrant. The gastrosplenic and splenorenal ligaments, two of the spleen’s ligaments, maintain the spleen’s normal anatomic position(26).
CT and ultrasound are the primary modalities that radiologists use for imaging the spleen. In some instances, MRI can be helpful.
The adult spleen’s average signal on MRI is hyperintense on T2-weighted imaging. On T1-weighted imaging, the spleen is hypointense relative to the liver(27). Deviations from this pattern can reflect iron overload disease processes, including hemochromatosis and hemosiderosis.
Pancreas
Using MRI for target volume delineation in pancreatic cancer has also resulted in smaller target volumes and reduced the interobserver variation. This occurrence is likely due to the improved soft-tissue contrast(28-29).
Recently, a research group published specific MRI-based GTV and OAR contouring recommendations in pancreatic cancer(30-31).
Pancreatic ductal adenocarcinoma is a typically malignant tumor. This condition, which accounts for 85% to 90% of all malignant pancreatic tumors, is the fourth most common cause of cancer death worldwide(32).
The remaining tumors of the pancreas are a diverse group of pancreatic neoplasms. These abnormal tissue masses comprise endocrine tumors, cystic pancreatic neoplasms, and other uncommon pancreatic tumors(33).
- Lukovic, J., Henke, L., Gani, C., Kim, T. K., Stanescu, T., Hosni, A., Lindsay, P., Erickson, B., Khor, R., Eccles, C., Boon, C., Donker, M., Jagavkar, R., Nowee, M. E., Hall, W. A., Parikh, P., & Dawson, L. A. (2020). MRI-Based Upper Abdominal Organs-at-Risk Atlas for Radiation Oncology. International journal of radiation oncology, biology, physics, 106(4), 743–753. https://doi.org/10.1016/j.ijrobp.2019.12.003
- Choi JY, Lee JM, Sirlin CB. CTand MR imaging diagnosis and staging of hepatocellular carcinoma: Part I. Development, growth, and spread: Key pathologic and imaging aspects. Radiology 2014;272:635-654.
- Saisho H, Yamaguchi T. Diagnostic imaging for pancreatic cancer: Computed tomography, magnetic resonance imaging, and positron emission tomography. Pancreas 2004;28:273-278.
- Lukovic, J., Henke, L., Gani, C., Kim, T. K., Stanescu, T., Hosni, A., Lindsay, P., Erickson, B., Khor, R., Eccles, C., Boon, C., Donker, M., Jagavkar, R., Nowee, M. E., Hall, W. A., Parikh, P., & Dawson, L. A. (2020). MRI-Based Upper Abdominal Organs-at-Risk Atlas for Radiation Oncology. International journal of radiation oncology, biology, physics, 106(4), 743–753. https://doi.org/10.1016/j.ijrobp.2019.12.003
- Henke L, Kashani R, Robinson C, et al. Phase I trial of stereotactic MR-guided online adapative radiation therapy (SMART) for the treatment of oligometastatic or unresectable primary malignancies of the abdomen. Radiother Oncol 2018;126:519-526.
- Acharya S, Fischer-Valuck BW, Kashani R, et al. Online magnetic resonance image guided adaptive radiation therapy: First clinical applications. Int J Radiat Oncol Biol Phys 2016;94:394-403.
- Mutic S, Dempsey JF. The ViewRay system: Magnetic resonanceguided and controlled radiotherapy. Semin Radiat Oncol 2014;24: 196-199.
- Werensteijn-Honingh AM, Kroon PS, Winkel D, et al. Feasibility of stereotactic radiotherapy using a 1.5T MR-linac: Multi-fraction treatment of pelvic lymph node oligometastases. Radiother Oncol 2019;134:50-54.
- Rosenberg SA, Henke LE, Shaverdian N, et al. A multi-institutional experience of MR-guided liver stereotactic body radiation therapy. Adv Radiat Oncol 2018;4:142-149.
- Palacios MA, Bohoudi O, Bruynzeel AME, et al. Role of daily plan adaptation in MR-guided stereotactic ablative radiation therapy for adrenal metastases. Int J Radiat Oncol Biol Phys 2018;102:426-433.
- Rudra S, Jiang N, Rosenberg SA, et al. Using adaptive magnetic resonance image guided radiation therapy for treatment of inoperable pancreatic cancer. Cancer Med 2019;8:2123-2132.
- Lukovic, J., Henke, L., Gani, C., Kim, T. K., Stanescu, T., Hosni, A., Lindsay, P., Erickson, B., Khor, R., Eccles, C., Boon, C., Donker, M., Jagavkar, R., Nowee, M. E., Hall, W. A., Parikh, P., & Dawson, L. A. (2020). MRI-Based Upper Abdominal Organs-at-Risk Atlas for Radiation Oncology. International journal of radiation oncology, biology, physics, 106(4), 743–753. https://doi.org/10.1016/j.ijrobp.2019.12.003
- Henke L, Kashani R, Robinson C, et al. Phase I trial of stereotactic MR-guided online adapative radiation therapy (SMART) for the treatment of oligometastatic or unresectable primary malignancies of the abdomen. Radiother Oncol 2018;126:519-526.
- Fast M, van de Schoot A, van de Lindt T, et al. Tumor trailing for liver SBRT on the MR-Linac. Int J Radiat Oncol Biol Phys 2019;103: 468-478.
- Keall PJ, Barton M, Crozier S. Australian MRI-Linac program, including contributors from Ingham Institute, Illawarra Cancer Centre, Liverpool Hospital, Stanford University, Universities of Newcastle, Queensland, Sydney, Western Sydney, and Wollongong. The Australian magnetic resonance imaging-linac program. Semin Radiat Oncol 2014;24:203-206.
- Fallone BG. The rotating biplanar linac-magnetic resonance imaging system. Semin Radiat Oncol 2014;24:200-202.
- Lukovic, J., Henke, L., Gani, C., Kim, T. K., Stanescu, T., Hosni, A., Lindsay, P., Erickson, B., Khor, R., Eccles, C., Boon, C., Donker, M., Jagavkar, R., Nowee, M. E., Hall, W. A., Parikh, P., & Dawson, L. A. (2020). MRI-Based Upper Abdominal Organs-at-Risk Atlas for Radiation Oncology. International journal of radiation oncology, biology, physics, 106(4), 743–753. https://doi.org/10.1016/j.ijrobp.2019.12.003
- Jabbour SK, Hashem SA, Bosch W, et al. Upper abdominal normal organ contouring guidelines and atlas: A Radiation Therapy Oncology Group consensus. Pract Radiat Oncol 2014;4:82-89.
- Goodman KA, Regine WF, Dawson LA, et al. Radiation Therapy Oncology Group consensus panel guidelines for the delineation of the clinical target volume in the postoperative treatment of pancreatic head cancer. Int J Radiat Oncol Biol Phys 2012;83:901-908.
- Lukovic, J., Henke, L., Gani, C., Kim, T. K., Stanescu, T., Hosni, A., Lindsay, P., Erickson, B., Khor, R., Eccles, C., Boon, C., Donker, M., Jagavkar, R., Nowee, M. E., Hall, W. A., Parikh, P., & Dawson, L. A. (2020). MRI-Based Upper Abdominal Organs-at-Risk Atlas for Radiation Oncology. International journal of radiation oncology, biology, physics, 106(4), 743–753. https://doi.org/10.1016/j.ijrobp.2019.12.003
- Lukovic, J., Henke, L., Gani, C., Kim, T. K., Stanescu, T., Hosni, A., Lindsay, P., Erickson, B., Khor, R., Eccles, C., Boon, C., Donker, M., Jagavkar, R., Nowee, M. E., Hall, W. A., Parikh, P., & Dawson, L. A. (2020). MRI-Based Upper Abdominal Organs-at-Risk Atlas for Radiation Oncology. International journal of radiation oncology, biology, physics, 106(4), 743–753. https://doi.org/10.1016/j.ijrobp.2019.12.003
- Lukovic, J., Henke, L., Gani, C., Kim, T. K., Stanescu, T., Hosni, A., Lindsay, P., Erickson, B., Khor, R., Eccles, C., Boon, C., Donker, M., Jagavkar, R., Nowee, M. E., Hall, W. A., Parikh, P., & Dawson, L. A. (2020). MRI-Based Upper Abdominal Organs-at-Risk Atlas for Radiation Oncology. International journal of radiation oncology, biology, physics, 106(4), 743–753. https://doi.org/10.1016/j.ijrobp.2019.12.003
- Dawson LA, Brock K, Moulton C, et al. Comparison of liver metastases volumes on CT, MR, and FDG PET imaging to pathological resection using deformable image registration. Int J Radiat Oncol Biol Phys 2007;69:S68.
- Coenegrachts K. (2009). Magnetic resonance imaging of the liver: New imaging strategies for evaluating focal liver lesions. World journal of radiology, 1(1), 72–85. https://doi.org/10.4329/wjr.v1.i1.72
- Lodge JP. Modern surgery for liver metastases. Cancer Imaging. 2000;1:77–85
- Coffey W, Balasubramanya R. Spleen Imaging. [Updated 2020 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554559/
- Ito K, Mitchell DG, Honjo K, Fujita T, Uchisako H, Matsumoto T, Matsunaga N, Honma Y, Yamakawa K. MR imaging of acquired abnormalities of the spleen. AJR Am J Roentgenol. 1997 Mar;168(3):697-702.
- Gurney-Champion OJ, Versteijne E, van der Horst A, et al. Addition of MRI for CT-based pancreatic tumor delineation: A feasibility study. Acta Oncol 2017;56:923-930.
- Li J, Denniston KA, Hussain SM, et al. Comparison of CT and MRIbased gross tumor volume and organ at risk delineation for pancreatic cancer patients undergoing neoadjuvant stereotactic body radiation therapy. Int J Radiat Biol Phys 2014;90:S356.
- Heerkens HD, Hall WA, Li XA, et al. Recommendations for MRIbased contouring of gross tumor volume and organs at risk for radiation therapy of pancreatic cancer. Pract Radiat Oncol 2017;7:126-136.
- Hall WA, Heerkens HD, Paulson ES, et al. Pancreatic gross tumor volume contouring on computed tomography (CT) compared with magnetic resonance imaging (MRI): Results of an international contouring conference. Pract Radiat Oncol 2018;8:107-115.
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96.
- Ansari, N. A., Ramalho, M., Semelka, R. C., Buonocore, V., Gigli, S., & Maccioni, F. (2015). Role of magnetic resonance imaging in the detection and characterization of solid pancreatic nodules: An update. World journal of radiology, 7(11), 361–374. https://doi.org/10.4329/wjr.v7.i11.361