

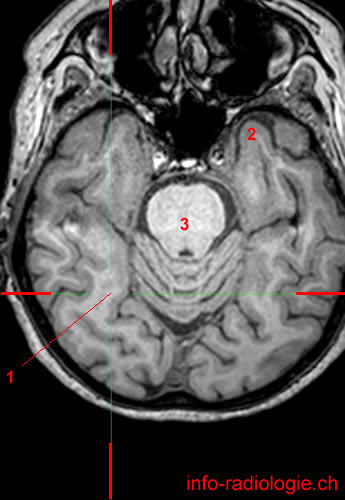
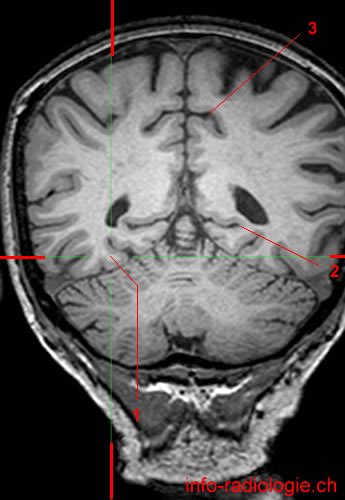
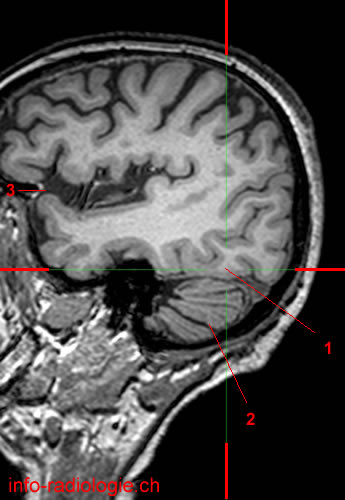
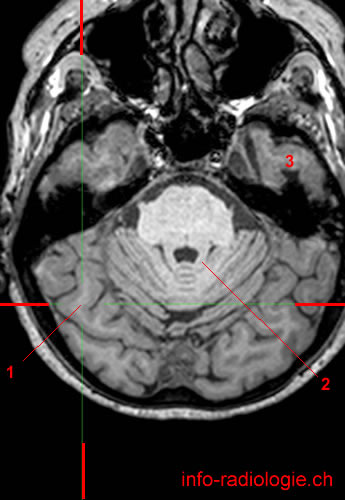
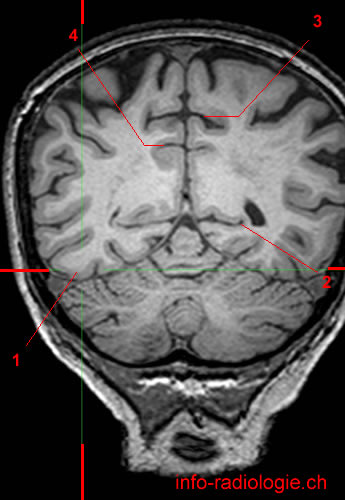
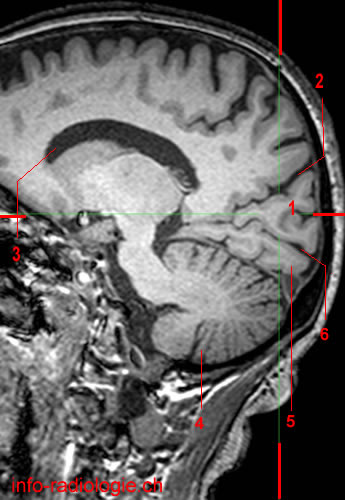
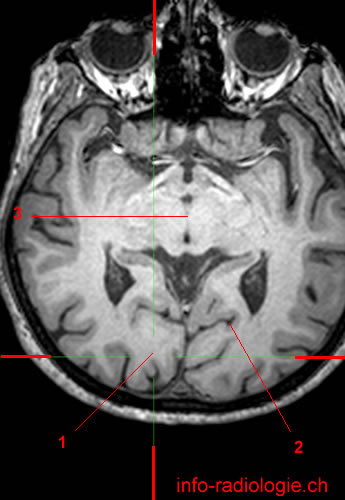
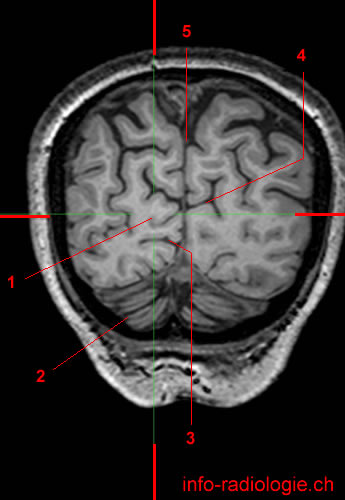
The occipital lobe is located in the posterior part of the cerebral hemispheres:
- posterior to the temporal lobe and parietal lobe
- the occipital lobe is partially separated from the parietal lobe by the parietooccipital fissure.
- In addition, there is only virtual separation between the temporal lobe and occipital lobe.
Anatomy of the Occipital Lobe
The brain’s two cerebral hemispheres are divided into four lobes: the frontal, temporal, parietal, and occipital lobes(1).
Reasoning, emotional regulation, and planning happen in the brain’s frontal lobe. The parietal lobe integrates sensory information, like pain, touch, temperature, and pressure(2).
The temporal lobe is dedicated to processing sensory information, such as recognizing language, forming memories, and hearing(3).
The occipital lobe is the smallest among the four lobes(4). This lobe is located underneath the occipital bone or the trapezoid-shaped bone at the lower back of the skull(5).
The occipital lobe covers 12% of the neocortex, which is involved in cognition, reasoning, motor skills, and sensory perception(6). The right and left occipital lobes are separated by a cerebral fissure(7).
The parietal lobe, temporal lobe, and occipital lobes are medially separated by a deep groove called the parieto-occipital sulcus(8). In the lateral exterior of the occipital lobe, there are three characteristic occipital sulci (grooves or depressions)(9):
- Transverse occipital sulcus
- Intraoccipital sulcus
- Lateral occipital sulcus
The transverse occipital sulcus is posteriorly located to the parieto-lateral occipital sulcus and crosses the brain’s superolateral area. In contrast, the intraoccipital sulcus is the extension of the parietal lobes’ intraparietal sulcus(10).
The lateral occipital sulcus divides the lateral occipital surface horizontally into inferior and superior gyri(11). These gyri convene and form the occipital pole (posterior end of the occipital lobe).
Extending from the parieto-occipital sulcus to the occipital pole is the calcarine sulcus or the calcarine fissure. The lower and upper banks of this sulcus contain the primary visual cortex(12).
The occipital lobe mainly serves as a visual processing area of the brain(13). This lobe functions by analyzing shapes, movements, and colors(14).
Visual information is sent from the brain’s contralateral half to each primary visual cortex(15). This cortex is divided into two pathways, the dorsal and ventral stream(16).
The dorsal stream is associated with object location and carries visual information to the parietal lobe. Meanwhile, the ventral stream transmits visual information related to object recognition to the temporal lobe(17).
The left occipital lobe interprets signals from the right visual space, while the right occipital lobe interprets signals from the left visual area(18).
Clinical Significance of the Occipital Lobe
An area of a wide variety of lesions, the occipital region of the brain plays an essential role in the central nervous system (CNS)(19).
Different occipital lobe injuries happen because of trauma, seizures, infections, neoplastic lesions, and vascular insults(20).
Homonymous hemianopia is a visual disorder that allows only one side of the eye to see(21). This disorder may be caused by stroke, inflammation, tumor, or brain injuries(22).
Contralateral homonymous hemianopia is caused by unilateral occipital lesions(23). This condition is a visual defect concerning the same sides of both eyes contralateral or opposite to the lesion(24).
Moreover, the occipital pole’s dual blood supply by the posterior and middle artery causes the homonymous hemianopia with macular sparing(25).
Posterior occipital lesions can also cause homonymous hemianopia with the limiting of crescent-shaped temporal vision(26).
Another disorder associated with the occipital lobe is Anton syndrome, which may occur in patients with cortical blindness(27).
Cortical blindness is due to the insult to the occipital cortex. This rare, neurological condition may result in binocular vision loss(28).
Anton syndrome is the denial of loss of vision (visual anosognosia), which is linked with confabulation (the presence of memories of experiences and events that never took place)(29).
This neurological visual impairment may lead to brain damage because of eye abnormalities(30).
Anton syndrome is characterized by total blindness, motion blindness (does not appreciate moving objects), or visual hallucinations due to the Charles Bonnet syndrome(31).
Another condition linked to occipital lobe injury is the Riddoch syndrome(32). People with Riddoch syndrome only see moving objects in the blind field, while non-moving things, colors, and shapes are invisible(33).
Occipital lobe epilepsy occurs when there are bright flashing lights and visual changes on the visual field’s left side (impairment occurs in the right cortex) or right side (impairment occurs in the left cortex)(34).
This condition is associated with blurring and eventual loss of vision, visual hallucinations, and rapid fluttering of eyelids or eye movements(35).
Additionally, a study suggested that changes in the occipital lobe, specifically in the white and gray matter, are associated with schizophrenia(36). However, the study also noted that further studies must be conducted to confirm this inference.
• Harnsberger HR, Osborn AG, Ross JS, Moore KR, Salzman KL, Carrasco CR, Halmiton BE, Davidson HC, Wiggins RH. Diagnostic and Surgical Imaging Anatomy: Brain, Head and Neck, Spine. 3rd ed. Salt Lake City, Utah. Amirsys. 2007.
• Bourjat P, Veillon F. Imagerie radiologique tête et cou. Paris, Vigot. 1995.
• Gouazé A, Baumann JA, Dhem A. Sobota. Atlas d’Anatomie humaine. Tome 3. Système nerveux central, système nerveux autonome, organe des sens et peau, vaisseaux et nerfs périphériques. 1er éd. Paris, Maloine. 1977.
• Kahle W, Cabrol C. Anatomie. Tome 3: Système nerveux et organe des sens. 1er éd. Paris, Flammarion. 1979.
- The University of Queensland Australia, (n.d.), Lobes of the Brain, retrieved from https://qbi.uq.edu.au/brain/brain-anatomy/lobes-brain
- Ibid.
- Ibid.
- Ibid.
- Rehman, A., Al Khalili, Y., Neuroanatomy, Occipital Lobe. [Updated 2020 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544320/
- Deyoe, E. A., (2002), Occipital Lobe, Encyclopedia of the Human Brain, retrieved from https://www.sciencedirect.com/topics/medicine-and-dentistry/occipital-lobe
- Rehman, A., Al Khalili, Y., Op. Cit.
- Ibid.
- Ibid.
- Ibid.
- Ibid.
- Ibid.
- Ibid.
- My MS Information on Multiple Sclerosis, (n.d.), Brain Anatomy: Lobes, retrieved from https://my-ms.org/anatomy_brain_part2.htm
- Rehman, A., Al Khalili, Y., Op. Cit.
- Ibid.
- Ibid.
- My MS Information on Multiple Sclerosis, (n.d.), Brain Anatomy: Lobes, retrieved from https://my-ms.org/anatomy_brain_part2.htm
- Flores, L. P., (December 2001), Occipital Lobe Morphological Anatomy, retrieved from https://www.scielo.br/scielo.php?script=sci_arttext&pid=S0004-282X2002000400010
- Rehman, A., Al Khalili, Y., Op. Cit.
- Cleveland Clinic, (n.d.), Homonymous Hemianopsia, retrieved from https://my.clevelandclinic.org/health/diseases/15766-homonymous-hemianopsia-
- Ibid.
- Rehman, A., Al Khalili, Y., Op. Cit.
- Ibid.
- Ibid.
- Ibid,
- Ibid.
- M Das J, Naqvi IA. Anton Syndrome. [Updated 2020 Oct 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538155/
- Ibid.
- Ibid.
- Ibid.
- Ibid.
- Ibid,
- John Hopkins Medicine, (n.d.), Focal Epilepsy, retrieved from https://www.hopkinsmedicine.org/health/conditions-and-diseases/epilepsy/focal-epilepsy#:~:text=Occipital%20lobe%20epilepsy%20is%20the,the%20occipital%20lobe%20are%20rare.
- Rehman, A., Al Khalili, Y., Op. Cit.
- Tohid, H., Faizan, M., & Faizan, U. (2015). Alterations of the occipital lobe in schizophrenia. Neurosciences (Riyadh, Saudi Arabia), 20(3), 213–224. https://doi.org/10.17712/nsj.2015.3.20140757