The pituitary gland is a small gland that controls the body’s hormones(1). A pituitary MRI or magnetic resonance imaging is a technique that takes pictures of the brain’s pituitary gland and its surrounding areas.
A systematic approach to the pituitary region is crucial as pituitary lesions may significantly alter a patient’s quality of life.
MRI is the modality of choice for hypothalamic-pituitary-related endocrine diseases(2). This modality uses a magnetic field, radio waves, and computer program to generate detailed image slices (cross-sections) of the head(3).
Soft tissue images allow the radiologist to evaluate and distinguish normal, healthy tissues from damaged ones.
Anatomy of the Pituitary Gland
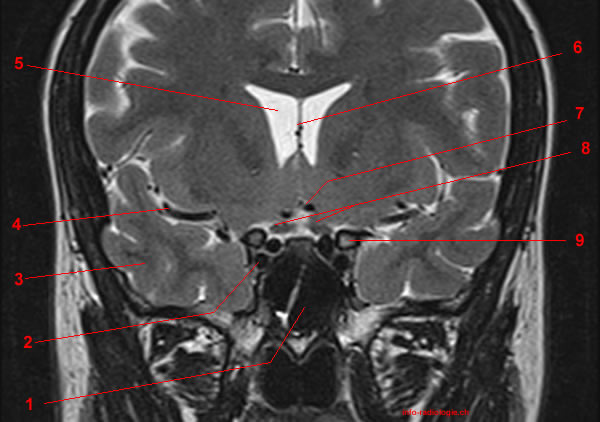
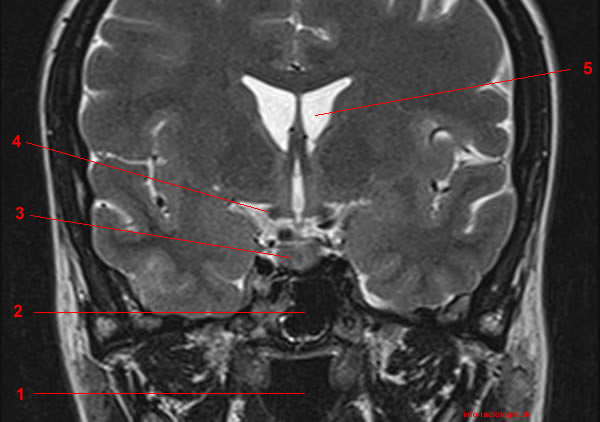
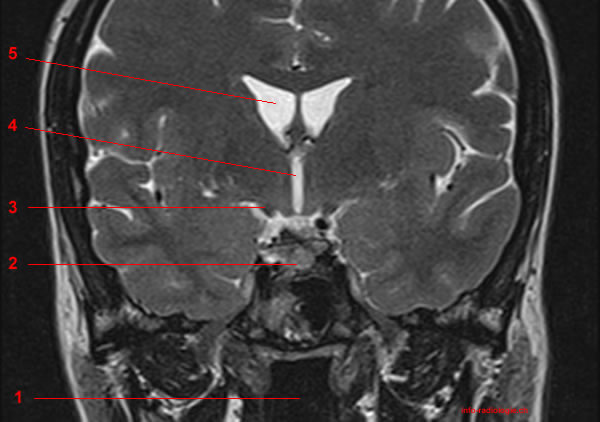
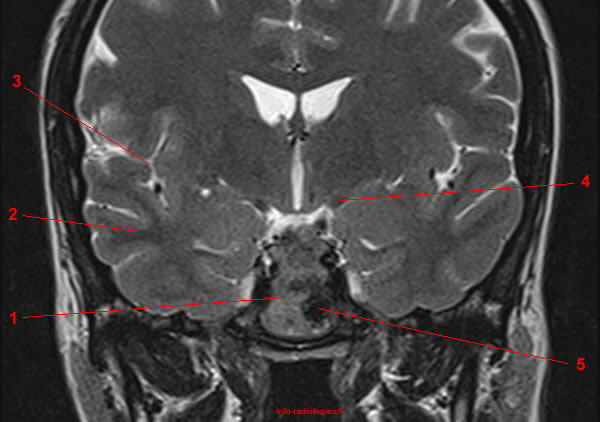
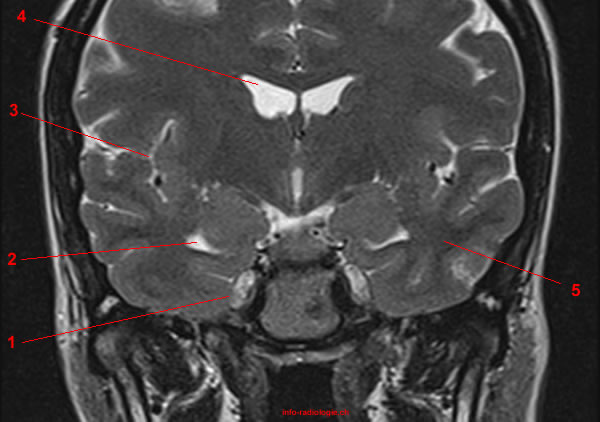
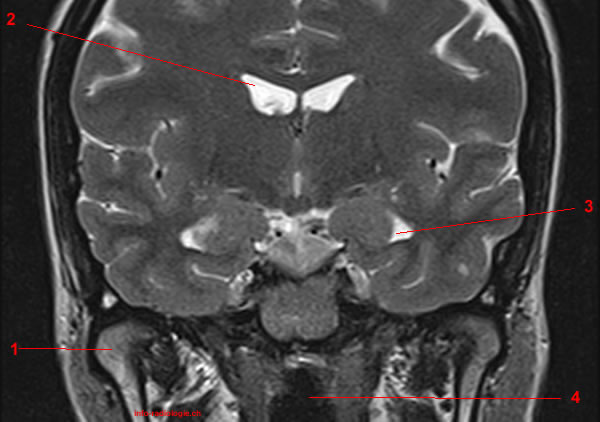
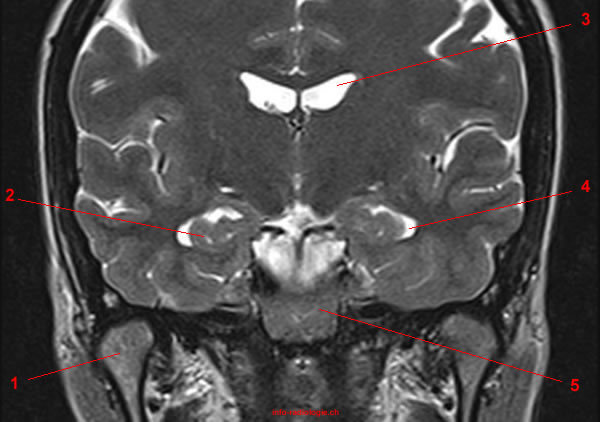
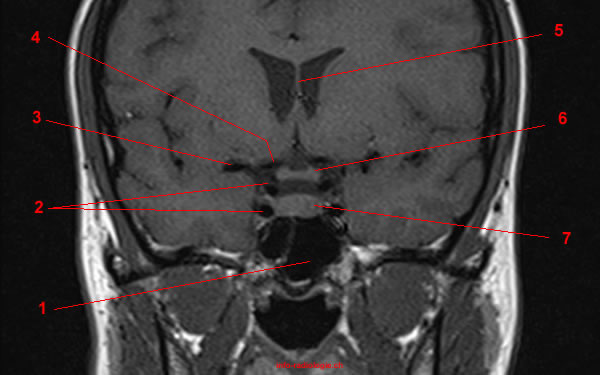
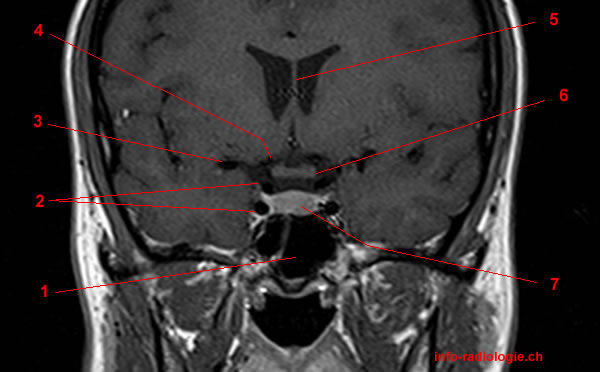
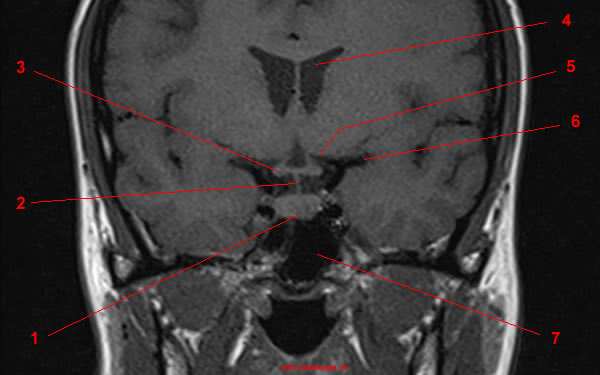
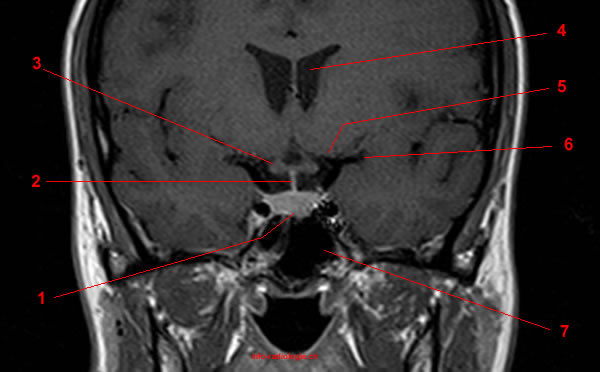
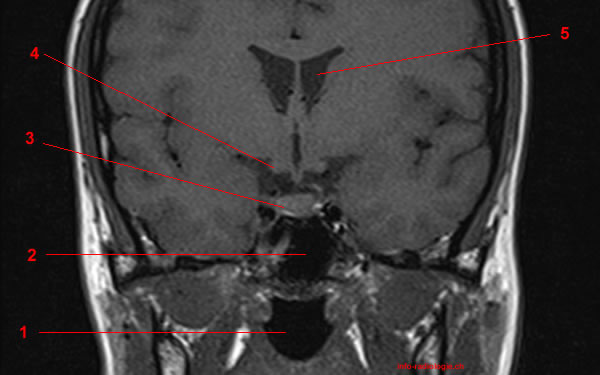
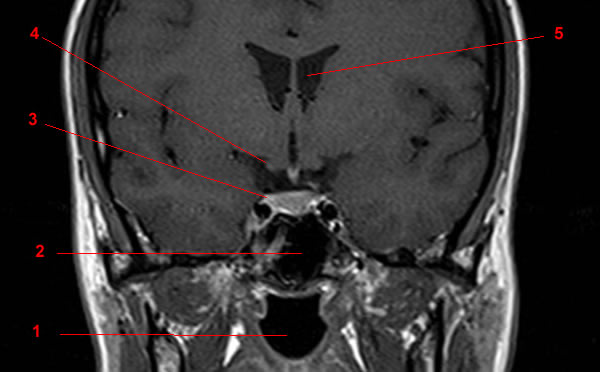
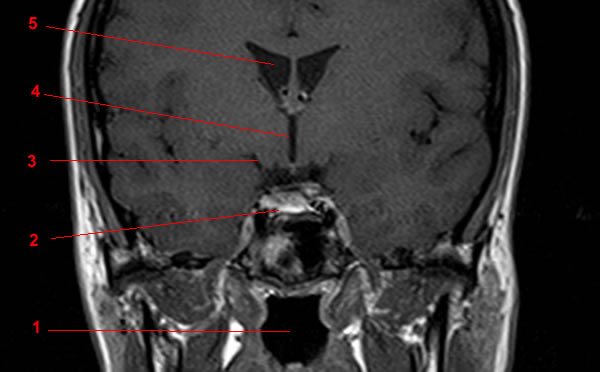
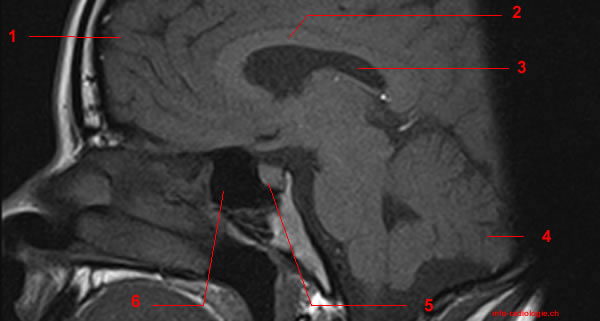
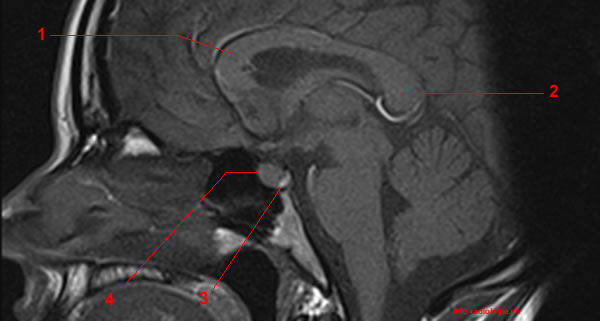
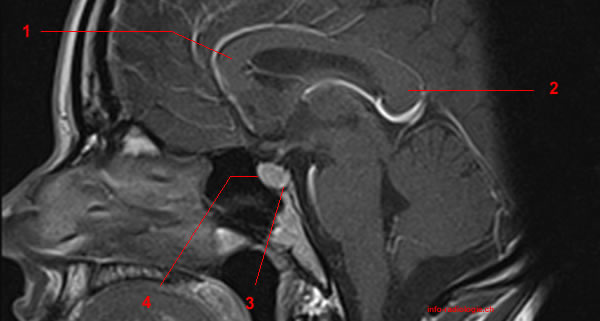
It is essential to clearly understand the pituitary gland anatomy and its surrounding structures for a successful assessment and interpretation of MR images.
The pituitary gland is located in the sella turcica of the sphenoid bone. This gland is anatomically and functionally related to the hypothalamus(4).
The hypothalamus is a brain region that extends from the anterior commissure to the posterior commissure. This region consists of multiple nuclei that regulate temperature, water balance, sexual activity, and drinking behavior(5).
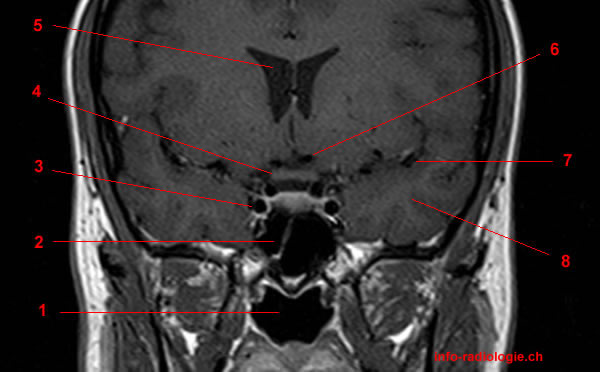
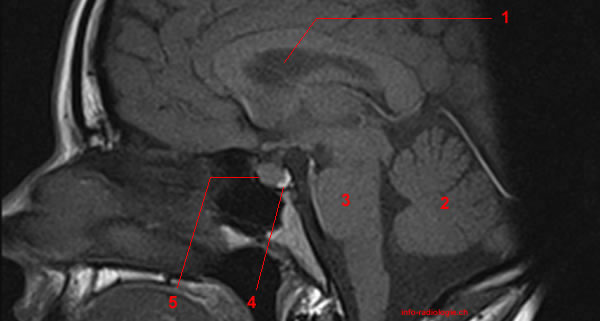
Two active lobes make up the pituitary gland: anterior (adenohypophysis) and posterior (neurohypophysis)(6).
The anterior lobe produces and secretes most pituitary hormones. Meanwhile, the posterior lobe releases two hormones initially produced in the hypothalamus’ nuclei.
On T1-weighted and T-2 weighted MR images, the anterior lobe is isointense (abnormality is similar to a reference structure) to the cortical brain. Meanwhile, the posterior lobe appears as a bright spot on T-1 weighted images(7).
Pituitary MR Imaging Techniques
MRI is the modality of choice for pituitary gland-related pathologies due to its superior soft-tissue contrast, lack of ionizing radiation, and multiplanar capability(8).
Additionally, MRI provides valuable information about the relationship of the gland with adjacent anatomical structures(9). This knowledge helps doctors plan medical or surgical strategies.
MR imaging aims to obtain a high spatial resolution image with a reasonable signal-to-noise ratio. It is important to have an accurate diagnostic differentiation of these lesions for effective and safe disease management(10).
Various advanced MR imaging techniques help evaluate and diagnose pituitary gland-related conditions.
Dynamic Contrast-Enhanced MRI
Dynamic contrast MRI proves to be the best imaging tool in evaluating pituitary adenomas(11). A fast turbo spin-echo sequence (TSE) or a three-dimensional transformation gradient-echo may be used for a more dynamic study.
This MRI technique usually requires a contrast medium of intravenous gadolinium (chemical-based dye) to improve the images’ clarity(12).
After a bolus injection of gadolinium, six consecutive sets of three images are obtained in the coronal (frontal) plane every ten seconds(13).
Aside from evaluating the pituitary microadenomas, dynamic contrast MRI has an important role in assessing the macroadenomas (benign tumor). This technique differentiates residual or recurrent tumors from postoperative tissues(14).
MR imaging can differentiate lymphocytic hypophysitis (LH) from nonsecreting macroadenomas. MR features indicative of LH include(15):
- Symmetric enlargement of the gland
- Homogeneous appearance
- Intense contrast enhancement
- Thickening and enhancement of the pituitary stalk
- Loss of posterior pituitary bright spot
- Enhancement of dura adjacent to the pituitary mass
- Intact sellar floor
3-Tesla (3T) MRI
3-Tesla MRI with stronger magnetic field strength offers an improved image quality. This technique also has enhanced spatial resolution with subtle differences between normal and abnormal tissue(16).
According to a recent study, preoperative localization of pituitary microadenomas in Cushing’s disease (hormonal disorder) is relatively better with 3T MRI(17).
The knowledge of average pituitary gland volume and pituitary stalk’s imaging appearance is vital in diagnosing different lesions.
3T MRI provides an accurate assessment of the pituitary stalk and subtle gland volume changes(18).
Magnetization Transfer (MT)
Magnetization transfer (MT) imaging is a recent advancement in the imaging field. This technique is useful for preoperative and postoperative assessment of pituitary adenomas in hyperprolactinemia patients(19).
In MT imaging, the tissue contrast is quantified by the magnetization transfer ratio (MTR) and depends mainly on the macromolecules’ concentration. Increased MTR values highly suggest persistent adenomatous tissue(20).
Radiologists can also use the MT technique in postoperative assessment and follow-up of patients with pituitary adenomas, especially when classical MRI is negative for residual tumor(21).
MT imaging’s prospect includes other pituitary disorders, such as precocious puberty and pituitary insufficiency(22).
Diffusion-Weighted Imaging (DWI)
Researchers have evaluated the role of diffusion-weighted imaging in the early detection of acute pituitary apoplexy. This condition results from either the hemorrhage or infarction of the pituitary gland(23).
A study noted that DWI assists in the early diagnosis of acute pituitary apoplexy with timely intervention and excellent outcomes(24).
Pituitary apoplexy may be diagnosed by the presence of peripheral contrast enhancement of an intrasellar mass and restricted water diffusion within the lesions on diffusion-weighted images(25).
Moreover, acute pituitary apoplexy on DWI may mimic pituitary hemorrhage, abscess, and hypophysitis(26).