Radiologists have historically imaged the male pelvis using many methods. Modalities range from conventional cystography, excretory urography, and retrograde urethrography to computed tomography and sonography(1).
However, in the study, the initial expectations of each method exceeded the long-term results. Thus, experts believe that the specificity and sensitivity of these methods are inferior in detecting and staging pelvic malignancies(2-6).
MRI Process
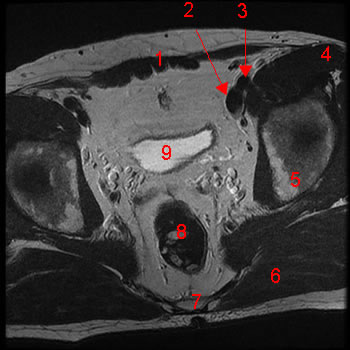
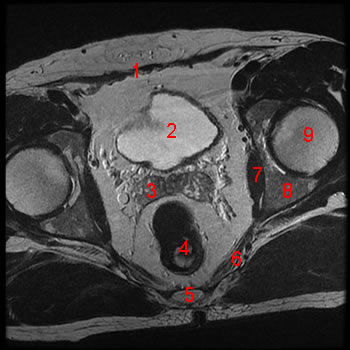
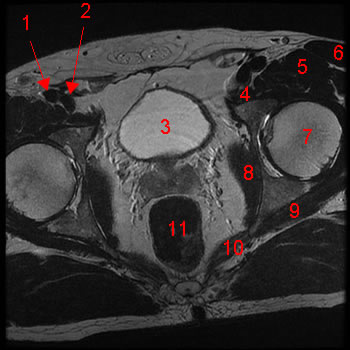
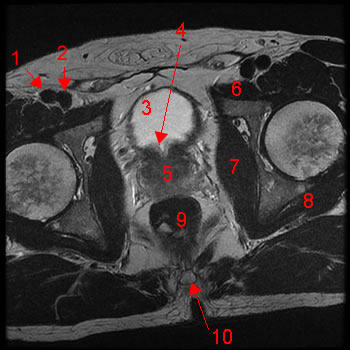
Magnetic resonance imaging (MRI) devices can provide direct transverse, sagittal, and coronal plane images. The different views are advantageous to clinicians assessing different pathologies related to the male pelvis(7).
MRI is a medical imaging method that uses a magnetic field and computer-generated radio waves to produce detailed images of body organs and tissues(8).
Prostate
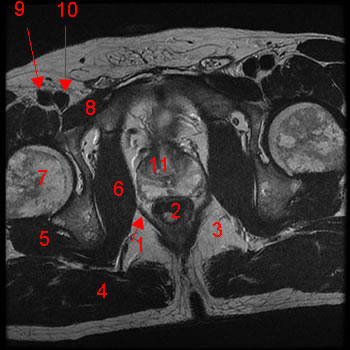
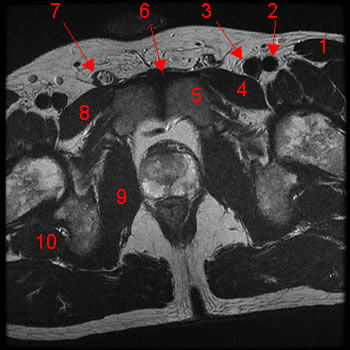
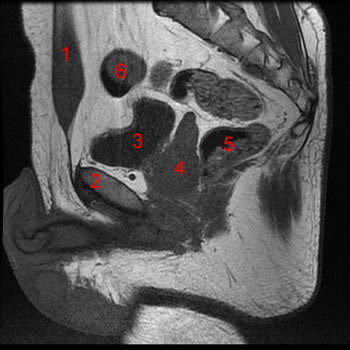
MRI can see the prostate gland upon using combined multiplanar images. Images can identify the prostate gland’s relations with the bladder floor and the rectum(9).
MRI scans can be used to detect prostate carcinoma. Prostate carcinoma is the most common cancer among males. Among the American male population, prostate carcinoma is the second most lethal malignancy(10).
To clarify, MRI has no direct role as a screening method for prostatic carcinoma due to the process being expensive and time-consuming. MRI also cannot differentiate benign from malignant diseases(11).
Still, MRI can detect early prostatic cancers in patients with existing tumors. MRI can also accurately stage these tumors(12).
Meanwhile, multiparametric-magnetic resonance imaging (mp-MRI) has shown promising results in the diagnosis, localization, risk stratification, and staging of clinically significant prostate cancer(13).
Mp-MRI can also reduce the number of missed clinically significant cancers and improve risk stratification. Therefore, this modality provides a more accurate therapeutic option for patients.
Bladder
Urine bladders may have to be distended or swollen for imaging purposes. Urine’s signal intensity varies with different spin-echo images(14).
MRI has the potential to become useful in finding the depth of wall invasion in tumors confined to the bladder(15). When extravesical tumors (tumors existing outside of the urinary bladder) are involved, MRI can be comparable to computed tomography (CT) in bladder tumor staging.
Additionally, MRI’s role in diagnosing and local staging of bladder cancer continues to evolve(16). Urinary bladder cancer is a heterogeneous disease and the fourth most common cancer among males and the tenth among females.
While early detection is essential, urinary bladder cancer has a high recurrence rate. As such, long-term surveillance after initial therapy is necessary(17).
The new emerging MRI sequences, diffusion-weighted and contrast-enhanced, are highly reliable for accurate local staging of urinary bladder cancer. This non-invasive modality is similar to conventional cystoscopy. Clinicians may use this method to efficiently evaluate patients with hematuria (blood in urine) from the lower urinary tract(18).
Genital Organs
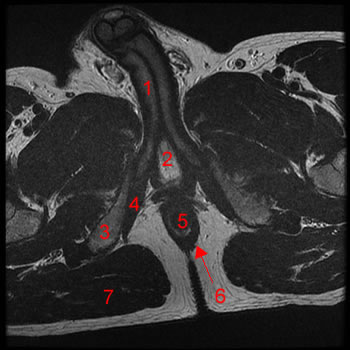
MRI can capture images of the penis’ corpora cavernosa from their connection to the ischia below the urogenital diaphragm. MRI can also display the inguinal canal and distinguish between the ductus deferens and internal spermatic vessels(19).
Furthermore, at medium intensity, MRI can take images of the testis. However, it does not observe a definitive distinction between the testis and epididymis (a convoluted duct behind the testis, along which sperm passes to the ductus deferens)(20).
MRI of the penis can show many essential structures and help assess penile cancer, priapism (persistent and painful penile erection), penile fibrosis, and Peyronie’s disease. However, this modality is sometimes inferior to clinical examination or ultrasound(21).
In terms of penile cancer, MRI can help detect bulky lymph nodes that warrant neoadjuvant chemotherapy (NACT) and potentially identify extranodal extension. MRI is also valuable in identifying the deep invasion of locally recurrent tumors, granting insight into the basis of treatment(22).
Rectum
Although MRI is not always available(23), the modality can image in different planes and is the dominant pelvic imaging method in assessing rectal cancer(24-27).
The main reason for MRI’s superiority is the excellent soft-tissue contrast between tumors and other soft tissues on T2-weighted imaging on MRI. Meanwhile, computed tomography (CT) has difficulties in this regard(28).
Magnetic resonance imaging is valuable in planning the treatment of rectal cancer. The modality is the superior technology in the local staging of patients with rectal cancer(29).
In the context of multidisciplinary meetings with standard terminology, MRI provides reliable risk allocation for different patient groups, helping them choose between different treatment regimens(30).
Despite the several limitations in rectal cancer staging, especially for lymph node staging, MR techniques in rectal cancer staging are continuously improving.
The role of MRI after preoperative treatment needs standard definition and evaluation. Still, MRI has proven its role in patients with local recurrence(31).