

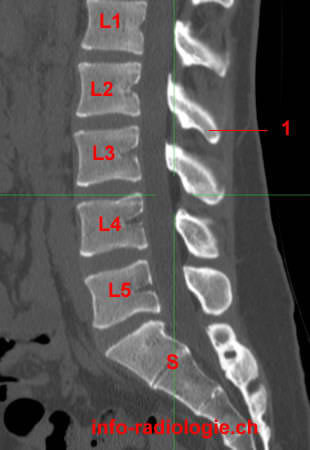
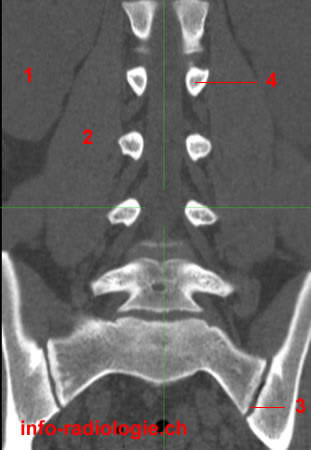
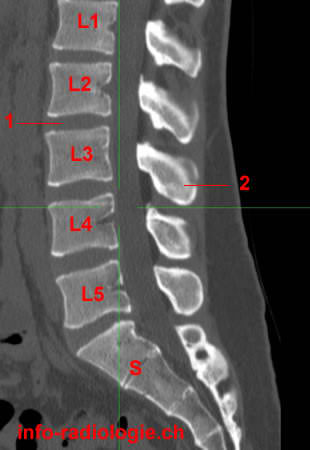
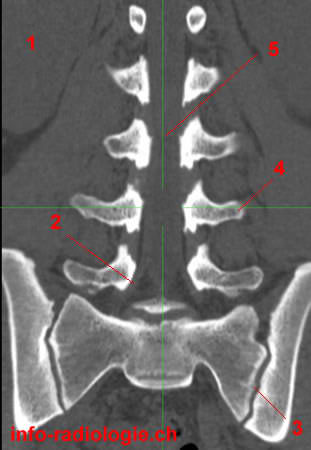
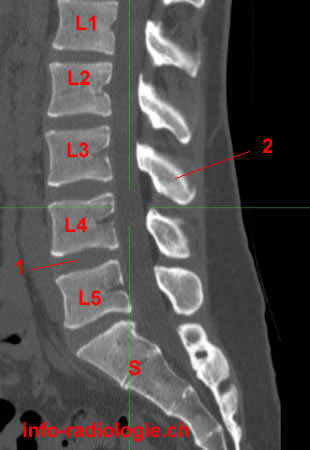
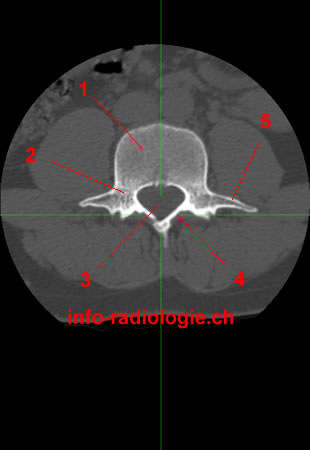
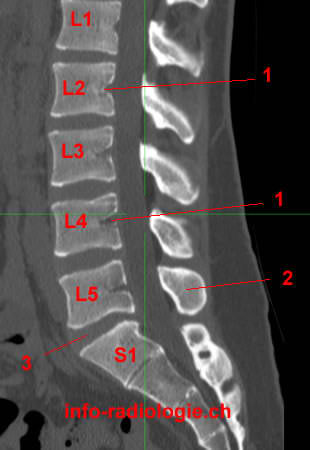
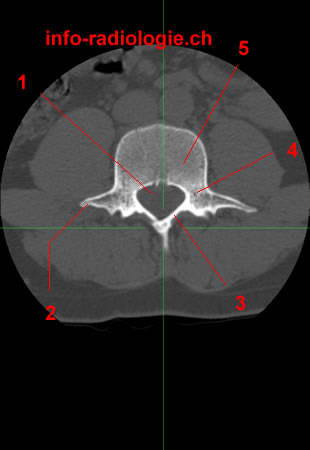
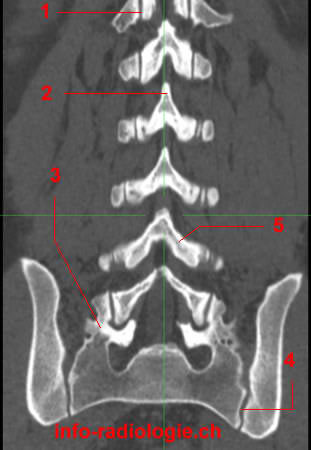
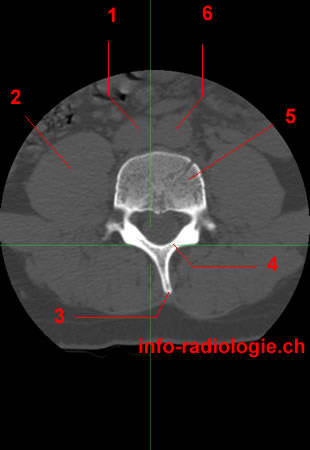
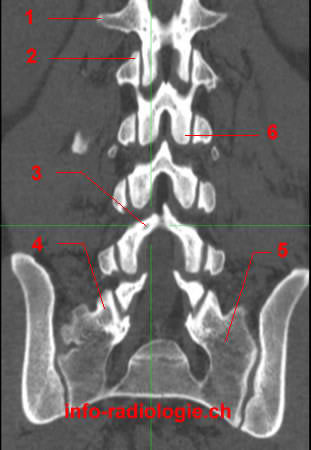
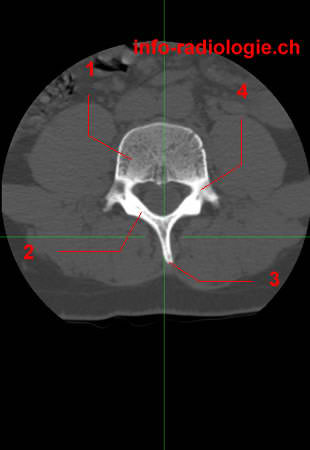
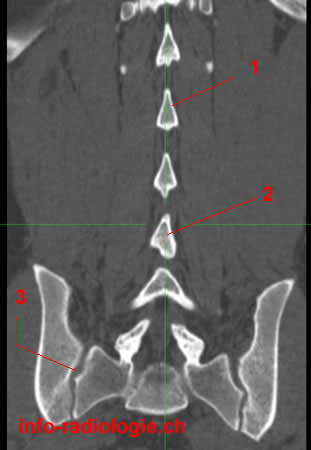
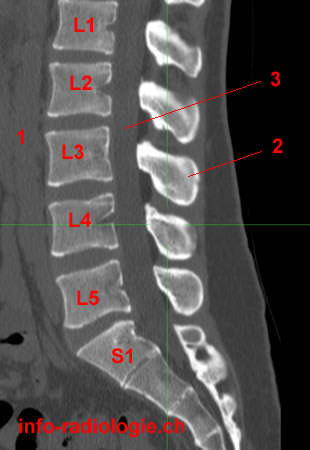
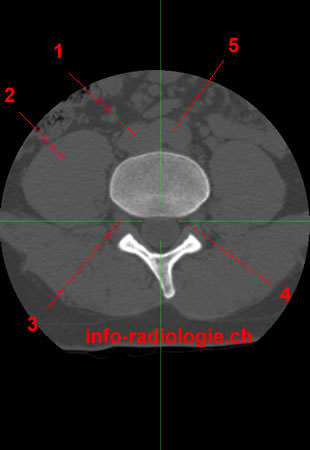
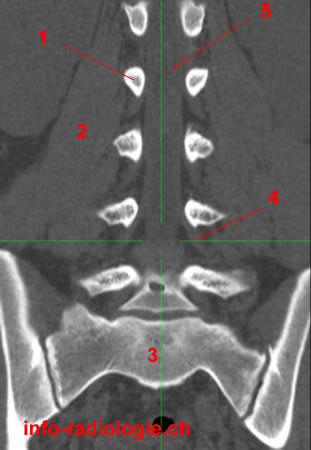
The images below are reconstructions obtained from a scan of lumbar spine. Each row of three thumbnails correspond to a given level and the green cross indicates the reference planes for each image of this Level.








Computed tomography (CT) is a proven method for evaluating the lumbar spine. This imaging modality provides great bone detail for assessing trauma, non-displaced fractures, complex fractures, and scoliosis in pre-operative and post-operative patients(1).
Lower back pain is a pervasive symptom. In the United States, it is the second most common complaint mentioned during visits to a healthcare provider(2). Lower back pain accounted for 4.4% of emergency department visits from 2000 to 2016(3). Back pain’s lifetime prevalence is approximately 70% to 85%(4).
Lower back pain causes range from muscle spasms and disc protrusions to more severe conditions. Such ailments include discitis, osteomyelitis (spinal inflammation), and malignancy (cancer)(5).
Depending on the modality, imaging methods provide varied details on these conditions.
CT is beneficial after surgery to evaluate the surgical hardware and bone graft material. These details are not as well-assessed on magnetic resonance imaging (MRI)(6).
CT myelograms help patients with various spinal equipment and those who have a contraindication for MRI. These tests occur after instilling a radiopaque dye into the subarachnoid space via lumbar puncture under CT or fluoroscopy guidance(7).
The subarachnoid space consists of the cerebrospinal fluid (CSF), major blood vessels, and cisterns. Cisterns mean enlarged CSF pockets that occur due to the separation of the arachnoid mater from the pia mater based on the brain’s and the spinal cord surface’s anatomy(8).
CT scans are also necessary for diagnosing occult sites of CSF leak following lumbar spine surgery or trauma(9).
Contraindications for CT myelogram include pregnancy and other general contraindications for a lumbar puncture. Such factors include elevated intracranial pressure and severe bleeding disorders(10).
Technical Aspects
Many patients tolerate CT well. Computed tomography is a fast modality and an ideal examination for assessing the spine’s bone structures(11).
Assessment of the spine’s soft-tissue structures is often limited. Radiologists can also indicate augmentation processes with contrast medium administration(12).
The diagnostic performance and the perceived image quality depend on imaging parameter choices and display modes. Results also depend on post-processing, particularly the reformatting parameters and the reconstruction algorithm(13).
Despite CT being a robust imaging method in general, artifacts can occur. Common misrepresentations include streak artifacts and movement artifacts. These distortions occur because excessively high attenuation materials can cause problems during image interpretation(14).
Spinal CT involves high radiation doses, making radiation protection necessary. Depending on the clinical question, radiologists must adjust the imaging parameters to adhere to the as low as reasonably achievable (ALARA) principle(15).
Making spinal CT imaging a quick, simple, and highly reliable examination of high diagnostic value generally only needs a common-sense approach(16).
Patient Positioning
The chosen patient position for spinal CT imaging is supine. This position involves having the patient lie on their back(17).
The supine position ensures minimal respiratory movement of the spine. This position usually guarantees good patient comfort while minimizing patient movement(18).
If radiologists require other positions, they must stabilize and secure the patient from moving or falling from the CT table(19).
Radiologists must use padding to avoid pressure points, especially during interventional procedures(20).
Finally, radiologists must avoid respiratory compromise. If a patient is sedated or anesthetized, protecting the airways and monitoring vital parameters are necessary(21).
Scan Parameters
A radiologist’s choice in the imaging parameters determines the image quality and the radiation dose(22).
The best image quality generally requires examinations with high kilovoltage (kV) and milliampere-second (mAs) settings. Thin collimation (the method of keeping beams in a given area) and low pitch are other conditions for good image quality.
The disadvantage of these requirements is the patient’s relatively high exposure to radiation and increased examination time and tube loading(23).
Tube loading, or the amount of heat energy deposited during X-ray exposure, is no longer relevant in newer multidetector-row CTs (MD-CT)(24).
Older generation scanners use their technical ability to determine the collimation, pitch, and exposure factors(25).
The examination time can significantly affect image quality, as images from longer exams may become problematic due to the patient’s breathing and movement artifacts. Movement artifacts can render examinations non-diagnostic(26).
Confused or uncooperative patients may prioritize exam speed over top resolution(27).
Radiation Burden
The main challenge for newer generation MD-CT is to achieve images that allow accurate and confident diagnosis while avoiding excessive exposure to radiation(28).
Most radiologists prefer good image quality. High-quality images result in high diagnostic confidence, although lower-dose exams may already answer the clinical question(29).
Radiologists prefer “good–looking” high-dose imaging over still diagnostic imaging that is contrast-reduced and noisier(30). It is challenging to establish the minimum necessary dose for any given examination precisely.
Sensible audit use can help reduce the patient’s radiation burden without affecting the subjective image quality(31). Using imaging phantoms (objects that stand-in for human tissues) can help establish the minimal acceptable kV and mAs to obtain acceptable images(32).
- Balasubramanya R, Selvarajan SK. Lumbar Spine Imaging. [Updated 2020 Apr 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553181/
- Chou R, Deyo RA, Jarvik JG. Appropriate use of lumbar imaging for evaluation of low back pain. Radiol Clin North Am. 2012 Jul;50(4):569-85.
- Edwards J, Hayden J, Asbridge M, Gregoire B, Magee K. Prevalence of low back pain in emergency settings: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2017 Apr 04;18(1):143.
- Farshad-Amacker NA, Farshad M, Winklehner A, Andreisek G. MR imaging of degenerative disc disease. Eur J Radiol. 2015 Sep;84(9):1768-76.
- Balasubramanya R, Selvarajan SK. Lumbar Spine Imaging. [Updated 2020 Apr 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553181/
- Balasubramanya R, Selvarajan SK. Lumbar Spine Imaging. [Updated 2020 Apr 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553181/
- Pomerantz SR. Myelography: modern technique and indications. Handb Clin Neurol. 2016;135:193-208.
- Shafique S, Rayi A. Anatomy, Head and Neck, Subarachnoid Space. [Updated 2020 Aug 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557521/
- Malhotra A, Kalra VB, Wu X, Grant R, Bronen RA, Abbed KM. Imaging of lumbar spinal surgery complications. Insights Imaging. 2015 Dec;6(6):579-90.
- Balasubramanya R, Selvarajan SK. Lumbar Spine Imaging. [Updated 2020 Apr 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553181/
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Tins, B. Technical aspects of CT imaging of the spine. Insights Imaging 1, 349–359 (2010). https://doi.org/10.1007/s13244-010-0047-2
- Richards PJ, George J, Metelko M, et al. Spine computed tomography doses and cancer induction. Spine (Phila Pa 1976) 2010;35(4):430–433.
- Abul-Kasim K, Gunnarsson M, Maly P, et al. Radiation dose optimization in CT planning of corrective scoliosis surgery. Neuroradiol J. 2008;21:374–382.