Computed tomography (CT) of the thorax allows radiologists to assess thoracic disorders or chest abnormalities. CT provides useful diagnostic information that is not usually attainable by conventional noninvasive radiological techniques(1).
CT Technique
Radiologists must perform thoracic CT studies in suspended full inspiration (inhalation) whenever possible. Radiologists monitor each procedure, selecting appropriate scan levels depending on the condition under review(2).
Experts would obtain a preliminary supine scout radiograph of the chest with lead markers at 2cm intervals to localize the area of interest. They may administer intravenous contrast when they are studying a possible vascular lesion case or when separating vascular and nonvascular lesions are necessary.
Intravenous contrast for CT is the most commonly used contrast agent(3). The material uses iodine to enhance CT images.
Radiologists can obtain sustained enhancement with a rapid intravenous infusion of 300ml of Conray 30 (iothalamate meglumine 30%)(4).
The infusion may require approximately 7 minutes through an 18-gauge needle. Four minutes after commencing the infusion, at least five well-enhanced scans are obtainable.
Normal Anatomy
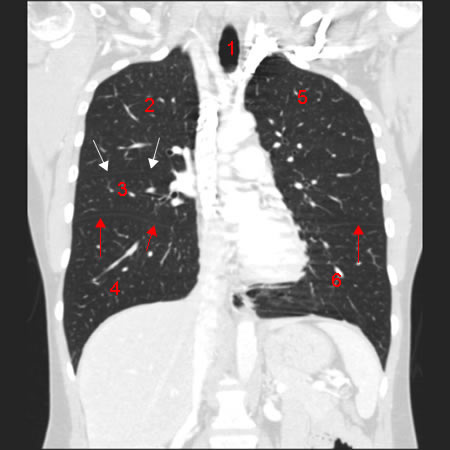
Cross-sectional CT scans give radiologists a unique perspective of the mediastinum(5), a division of the chest cavity containing the heart, thymus gland, parts of the esophagus, trachea, and other structures(6).
The modality may also identify structures that conventional radiographic techniques cannot separate(7).
The aorta is usually visible. A thin band of fat may separate the structure from other mediastinal structures. A rim of calcium may outline the aorta of elderly patients. Experts may similarly profile other vessels.
The esophagus is difficult to assess. This structure blends in with other mediastinal structures. During an assessment, examiners may see a small amount of air in the esophagus in approximately 40% of regular patients. In the hilar region (middle parts), the pulmonary arteries, veins, and airways are identifiable.
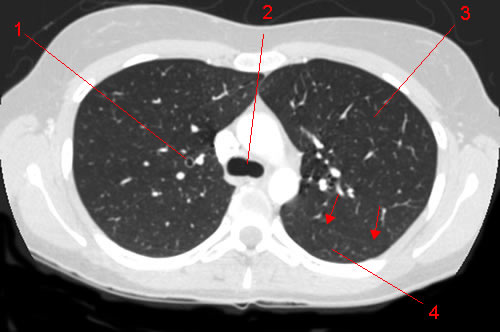
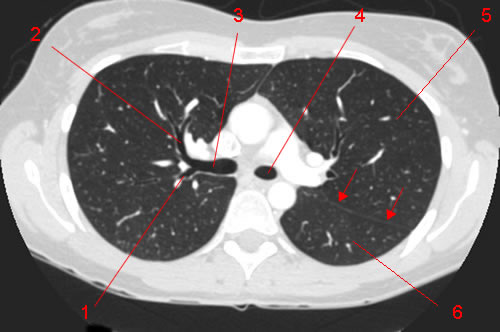
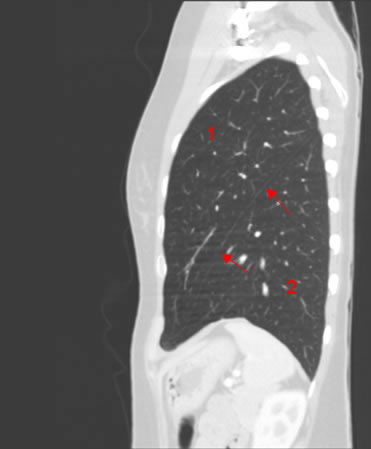
Radiologists require a different window width and level to see the lungs. In an appropriate setting, clinicians can demonstrate the status of different structures.
Such structures include the pulmonary parenchyma, the intrapulmonary vessels, and some normal bronchi.
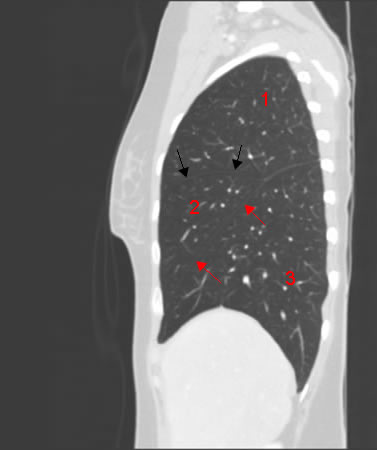
Like a standard chest radiograph, a CT scan has preferential pulmonary blood flow to the lung’s dependent portion (the lung’s dorsal portion in the supine position)(8).
Additionally, the degree of inspiration at the time of a conventional radiograph affects the chest’s normal transverse or horizontal anatomy.
Lung volume is smaller during expiration or exhalation. The mediastinum appears wider than usual, and the lung’s attenuation values are considerably higher. The parenchymal tissue’s resulting compression causes this condition.
Considering these changes are necessary for a radiologist’s evaluation of normal and pathologic thoracic anatomy.
Currently, there is limited information about the heart’s anatomy to cardiac motion during the scanning cycle. Still, respiratory gating techniques are promising for useful cardiac studies(9).
Clinical Uses of Thoracic CT Scanning
Radiologists have used CT to study a wide range of chest problems, with the mediastinum as the primary area of interest(10). Common clinical thoracic conditions that CT has helped assess may include the following:
Mediastinum
Attenuation Value Determination of Mass
Plain chest radiographs detecting mediastinal masses is a common diagnostic problem in the thorax. CT’s recognition of a mediastinal mass’ precise attenuation value may permit a definitive, noninvasive diagnosis(11).
Lesions presenting attenuation values characteristic of fatty tissue include a Morgagni hernia, Bokdalek hernia, and pericardial fat pad.
Evaluation of Mediastinal Widening
The mediastinal widening that plain chest radiographs identify may be due to a common variant such as fat, aorta aneurysm, or solid neoplasm.
CT scanning makes it possible to determine the cause for widening without needing more invasive procedures such as aortography(12).
Mediastinum widening is not always related to vessels or tumors. The widening may represent excessive fat deposition in the mediastinum, a diagnosis that CT can make immediately. This condition may occur in patients on steroid medications(13) or obese(14).
Evaluation of Paraspinal Widening
Paraspinal widening may present a diagnostic issue that clinicians find challenging to resolve with conventional techniques. In such clinical cases, radiologists may use CT to clarify abnormal widening causes(15).
Clinicians can identify the abnormal nodes when adenopathy (glandular tissue or lymph node inflammation) causes the widening.
CT can also diagnose other unexplained causes of widening in the paraspinal region, including aneurysms of the descending aorta, a direct extension of skeletal infection or tumor, and herniation of omental fat through the esophageal hiatus.
Lungs
Occult Disease
CT evaluates certain lung diseases possible, especially those virtually undetectable on conventional chest radiography images. CT can help evaluate patients with parenchymal disease that a surrounding pleural effusion (water on the lungs) may obscure(16).